

In contemporary societies, a fundamental understanding still exists that all people are heterosexuals. This phenomenon is often referred to as heteronormativity (Herek, 2004). One consequence of a heteronormative society is that it creates homonegative attitudes. Many men who have sex with men (MSM) must endure these attitudes from others, but as part of the same society, they themselves may hold the same attitudes. Negative attitudes toward homosexuality, or any devaluation of MSM executed by an individual, a group, or society, are referred to as homonegativity, homophobia, or internalized homophobia (Mayfield, 2001). Internalized homonegativity (IH) is defined as the extent to which an MSM has accepted and internalized society’s negative perceptions that his own homosexual attraction or behavior is bad, shameful, sinful, or imitating (Herek, 1996; Smolenski, Diamond, Ross, & Rosser, 2010). IH is characterized by an intrapsychic conflict between having same-sex sexual attraction and a desire to be heterosexual (Herek, 2004). According to Herek (2004), IH can be regarded as an expression of a sexual stigma. Sexual stigma is based on a collective devaluation of sexual minorities, assessed against heterosexuality as an expression of what is “normal.” Sexual stigma is created in an interaction process where the negative stereotypes and attitudes toward sexual minorities are learned and internalized during childhood and adolescence by cultural and group-specific socialization processes (Herek, Gillis, & Cogan, 2009). There is an expectation in society that individuals grow up to be heterosexuals. The sexual minority is seen as representing a deviation and is therefore hidden. This assumption affects all members of society, regardless of sexual orientation. Even if an individual belongs to a sexual minority, he/she can still hide his/her sexual orientation, which means everyone can potentially be heterosexual (Herek, 2004; Herek et al., 2009). Internalized sexual stigma can be defined as the personal acceptance of a sexual stigma as part of one’s own value system and self-concept (Herek et al., 2009). In heterosexuals, this is expressed in the form of negative attitudes toward sexual minorities. MSM who have grown up in such a culture have learned and internalized the same sexual stigma and may therefore also have negative attitudes toward other individuals from the homosexual minority. When an MSM’s negative attitudes and feelings toward homosexuals are directed at himself and his own behavior, it is referred to as self-stigmatization or IH.
IH and mental health
In a systematic review, Berg, Munthe-Kaas, and Ross (2016) found that over 200 studies had been conducted on IH during the 1989–2012 timeframe. Most studies on IH have focused on IH as a predictor of reduced mental health or reduced psychological well-being. A consistent finding in studies is that internalized homonegativity is clearly linked to depression among gay men (Feinstein, Goldfried, & Davila, 2012; Igartua, Gill, & Montoro, 2003; Newcomb & Mustanski, 2010; Meyer, 2003; Ross & Rosser, 1996; Rosser et al., 2008). In addition, in a study conducted on MSM in the USA, Ross and Rosser (1996) found that a higher degree of IH was significantly associated with dysthymia and the likelihood of being in therapy. Higher IH is also shown to be associated with negative self-confidence (Herek, Cogan, Gillis, & Glunt, 1998; Szymanski & Gupta, 2009), problems with interpersonal relations (Frost & Meyer, 2009), sensitivity regarding rejection (Pachankis, Goldfried, & Ramrattan, 2008), higher likelihood of being in conversion therapy (Tozer & Hayes, 2004), poor sexual health (Rosser et al., 2008), and risk behavior for HIV (Ross, Smolenski, Kajubi, Mandel et al., 2010). Research shows that compared to heterosexual men, more homosexual and bisexual men have had thoughts about committing suicide (Bakkeli & Elgvin, 2014) and have higher risk of committing suicide (Igartua et al., 2003; Meyer, 2003; Paul, Catania, Pollack, Moskowitz et al., 2002; Rüütel, Valk, & Lõhmus, 2017). These previous studies all pinpoint IH as an important factor for healthiness in MSM. However, most of the referred studies are conducted in another cultural context than the Norwegian one, and we do not know whether the same results apply to Norwegian MSM. What is known is that lesbian and bisexual women in a Norwegian survey reported relatively low levels of minority stress and IH (Prell & Træen, 2018), but whether the same result applies to MSM remains to be seen. Drawing on this background, the overall purpose of this paper is to study IH among MSM in Norway. Resting on a conceptual model, it is postulated that there is a relationship between IH and individual or socio-demographic factors (age, level of education, urbanity), psychological factors (affect status, sexual self-esteem, compulsive sexual behavior, sexual satisfaction), and social factors (openness about own sexual orientation, membership in organizations for homosexuals). This conceptual model is visualized in Figure 1. The reasons for selecting the factors included in the model will be outlined below.


IH and individual factors
Studies have shown a relationship between IH and age, and IH is higher among older MSM than in younger MSM (David & Knight, 2008; Grossmann, D’Augelli, & O’Connell, 2001; Kuyper & Fokkema, 2010). Older MSM are likely to have grown up and developed their sexual identity in a society with more prejudice against homosexuality than younger MSM are (Mayfield, 2001). Even though younger MSM were born in a society with more openness and acceptance toward sexual minorities, they still live in a heteronormative society. This is, for instance, reflected in the language, through terms like “coming out as homosexual” or “coming out of the closet,” to describe non-heterosexual orientation. In the period of life when sexual identity is developed and explored, deviation from the norm can be difficult. When this deviation is additionally stigmatized, one may reasonably expect higher IH in younger MSM. Further, in some cultures, younger MSM may be more troubled by rejection from their church and/or family than older MSM would be, because the latter may have come to terms with their preferences (Moleiro, Pinto, & Freire, 2013).
Higher levels of education are associated with more positive attitudes toward homosexuality and, accordingly, less IH (Lambert, Ventura, Hall, & Cluse-Tolar, 2006; Ross et al., 2010). Additionally, gay people with higher education reported being more socially comfortable in associating with homosexuals. This tendency was particularly so among younger segments of people with a high level of education. In a study conducted in the USA, homosexuals living in rural areas and smaller towns tended to report more experience with discrimination and greater social stigma than did those living in urban areas (Swank et al., 2012). Compared to people living in rural areas, those living in larger cities may have less prejudice because they have more experience in interacting with different types of people. They may therefore be more accustomed to dealing with a greater variety of opinions and lifestyles. Deviation from the heterosexual norm may be more difficult in smaller towns, and large-sized cities offer greater opportunities to find queer communities. It can therefore be assumed that MSM living in urban areas will have less IH than those living in rural areas will, because urban people may have fewer experiences of discrimination and stigma.
IH and psychological factors
Affective personality traits are thought to consist of two distinct and relatively independent dimensions, that is, positive affect (PA) and negative affect (NA) (Watson, Clark, & Tellegen, 1988). The PA dimension reflects the degree to which a person feels enthusiastic and active, and it expresses a disposition to maintain a positive outlook on the future and in different contexts (Norlander, Bood, & Archer, 2002; Watson et al., 1988). A high PA expresses a state of high energy, complete concentration, and commitment. Likewise, a low PA expresses sadness and lethargy. People who have high levels of PA often feel greater satisfaction with life and usually have more self-confidence (Norlander et al., 2002). The NA dimension is intended to capture a general dimension of subjectively experienced distress and anxiety, which involves a variety of aversive mood states such as anger, fear, and guilt. A low NA will be interpreted as a state of calmness (Watson et al., 1988). A person with high PA and low NA may have an affective interpretation framework that provides better conditions to face prejudice and stigma from both people and society.
Sexual self-esteem and sexual satisfaction refer to a person’s tendency to positively evaluate how he relates sexually to another person and the degree to which he experiences such relations as sexually satisfying (Snell, Fisher, & Walters, 1993). This definition implies that high sexual self-esteem is associated with fewer negative thoughts about one’s sexuality. For MSM, high sexual self-esteem is likely to be associated with fewer negative emotions (Træen, Noor, Grey, Iantaffi et al., 2014) and a reduced need for confirmation from others (Leary, Tchividjian, & Kraxberger, 1999). Thus, high sexual self-esteem should be associated with a low degree of IH. MSM who have not been socialized to be ashamed of their sexuality are likely to have fewer negative thoughts related to their sexuality and a higher sexual self-esteem than MSM with a high degree of IH do.
Compulsive sexual behavior can be defined as an inability to control one’s sexual urges and desires (Coleman, Miner, Ohlerking, & Raymond, 2001). For the individual, compulsive sexual behavior may cause a break in social relationships and difficulties in both job contexts and everyday life functioning (Finlayson, Sealy, & Martin, 2001; Kalichman & Cain, 2004). Smolenski, Ross, Risser, and Rosser (2009) found a moderate correlation between high IH and compulsive sexual behavior. However, it is unknown whether this finding goes beyond MSM in the USA. The present study contributes to shedding light on this relationship.
IH and social factors
Revealing that one belongs to a sexual minority may involve a risk of being exposed to hate crime or harassment. To avoid such exposure, many MSM choose to appear as a part of the heterosexual majority (Herek et al., 2009). The choice of this strategy is associated with higher levels of IH. Several studies have also shown that low openness about one’s sexual orientation with friends and family members is associated with higher levels of IH (Herek et al., 1997; Frost & Meyer, 2009; Pachankis et al., 2008; Rosser et al., 2008). It could be that not being open provides greater IH because the individual conceals a secret that may be associated with sin, shame, and self-stigma (Herek et al., 2009). Higher levels of IH in homosexuals are shown to be associated with feeling less affiliation to the lesbian, gay, bisexual, trans, and queer (LGBTQ) community. Herek et al. (1997) found that IH was negatively correlated with the degree to which MSM experienced being a part of the gay community, which in turn is an important part of their identity construction. It can reasonably be assumed that MSM with high IH feel less integrated in gay networks compared to MSM with low IH (Rosser et al., 2008). Further, gay men who were less comfortable with exposing their sexual orientation had fewer LGBTQ friends (D’Augelli, Hershberger, & Pilkington, 1998). A survey among older LGBTQ adults in the Netherlands found that having a social network in the LGBTQ community acted as a buffer against sexual minority stress. To feel belongingness to an LGBTQ community, it is necessary for the individual to have the opportunity to make a positive comparison, as opposed to comparing oneself to the majority’s heteronormative attitudes and stigma (Swank et al., 2012). Therefore, high IH and isolation from others in the same sexual minority may be correlated in Norwegian MSM.
Methods
Participants
The self-selected sample comprised of 529 Norwegian MSM who volunteered to participate in an online survey on the use of sexually explicit media (SEM) and sexual behaviors. To participate in the study, participants had to be Internet-using, male, and aged 18 years or over.
Procedure
Between January 15 and February 2, 2012, MSM were invited to participate in a survey about the use of pornography and sexual behavior through pop-up banners on Norway’s largest gay website ‘‘www.gaysir.no.’’ Participants were not compensated for their participation. The study was approved by the Norwegian Social Science Data Services Institutional Review Board.

The questionnaire used for the present online survey was adapted from an NIH-funded study of SEM consumption and HIV risk behavior among MSM in the USA (Rosser, Smolenski, Erickson, Iantaffi et al., 2013). The questionnaire contained questions about socio-demographic factors, membership in an organization for homosexuals, openness about one’s sexual orientation, sexual behavior, use of pornography, IH, affect status, sexual self-esteem, and compulsive sexual behavior. Of the 529 individuals who responded to the survey, 70.5% claimed to be homosexual, gay, or same-gender loving, 23.6% bisexual, 1.6% heterosexual, and 4.1% did not state their sexual identity (see Table 1). All men were included in the analyses in this study. About 65% of the MSM in the sample lived in cities, and they reported that most or all people they knew were aware of their sexual orientation. The majority of the sample had a university level of education, and 36% were members of an organization for LGBTQ persons. The mean age of the respondents was 34.7 years.

Measures
Internalized homonegativity was measured by “The revised reactions to homosexuality scale” (Smolenski et al., 2010). This is a seven-item short version of the original “Reaction to internalized homophobia scale” developed by Ross & Rosser (1996). Each item was evaluated on a 7-point scale from 1 = Strongly disagree to 7 = Strongly agree. As the background to Smolenski et al.’s (2010) study, three mean sum score variables were constructed: 1) “Personal comfort with a gay identity” (“Even if I could change my sexual orientation, I wouldn’t,” “I feel comfortable being a homosexual man,” “Homosexuality is as natural as heterosexuality;” Cronbach’s alpha =.70); 2) “Social comfort with gay men” (“I feel comfortable in gay bars,” “Social situations with gay men make me uncomfortable” (reversed); Cronbach’s alpha = .55); and 3) “Public identification as gay” (“I feel comfortable discussing homosexuality in a public situation,” “I feel comfortable being seen in public with an obviously gay person”; Cronbach’s alpha = .69). On all constructed variables, a higher score indicates a lower degree of IH.
Level of education was measured as 1 = Compulsory school, 2 = High school, 3 = Some college (no degree), 4 = Bachelor’s degree, 5 = Professional/Master’s degree, and 6 = PhD level. The variable was recoded into 1 = lower level of education (1–2), 2 = medium level of education (3–4), and 3 = higher level of education (5–6).
Membership in organizations for homosexuals was measured as 1 = “No,” 2 = “Yes,” and 3 = “Don’t know” The variable was recoded into 1 = “Yes” and 0 = “No” (previous categories 2 and 3).
Openness about one’s sexual orientation was measured by the question “Men vary in the degree to which they report being ‘out of the closet’ or open about being sexually attracted to other men. How ‘out’ are you about your sexual attraction to other men?” The response categories were 1 = Not “out” at all, 2 = “Out” to a few people I know, 3 = “Out” to about half the people I know, 4 = “Out” to most people I know, and 5 = “Out” to all or almost all people I know.
Affect status was measured by means of a 10-question version of the “Positive and negative affect schedule” (PANAS) (Thompson, 2007): “Indicate to what extent you have felt this way during the past three (3) months.” Positive affect (PA) was measured by the adjectives “Inspired,” “Excited,” “Enthusiastic,” and “Determined.” Negative affect was measured by “Scared,” “Distressed,” “Afraid,” “Alert,” “Upset,” and “Nervous.” All questions were evaluated on a scale from 1 = “Very little or not at all,” 2 = “A little,” 3 = “Moderately,” 4 = “Quite a bit,” and 5 = “Extremely.” Mean sum score variables were constructed, and a high score on the subscales indicates a higher degree of positive and negative affect, respectively. Cronbach’s alpha was 0.70 for PA and 0.85 for NA in this sample, which corresponds well to Thompson’s (2007) findings.
Sexual self-esteem was assessed using the scale developed by Snell et al. (1993). It comprises 10 different items listed under the heading “Please indicate how much the following items describe how you have felt about yourself in the last three months.” The following items were on the sexual self-esteem subscale: “I am confident about myself as a sexual partner,” “I am a pretty good sexual partner,” “I am better at sex than most other people are,” “I would rate myself pretty favorably as a sexual partner,” and “I would be very confident in a sexual encounter.” The sexual satisfaction subscale comprised the following items: “I am very satisfied with the way my sexual needs are currently being met,” “I am very satisfied with my sexual relationship(s),” “My sexual relationship(s) meets my original expectations,” “My sexual relationship(s) is very good compared to that of most others,” and “I am very satisfied with the sexual aspects of my life.” Each item was rated as 1 = not at all like me, 2 = only a little like me, 3 = somewhat like me, 4 = a lot like me, and 5 = exactly like me. We used the arithmetic mean of the 10 items to create a composite measure of sexual self-esteem. Higher scores on the composite measure indicate greater sexual self-esteem/sexual satisfaction. The Cronbach’s alpha of the sexual self-esteem and sexual satisfaction scales was 0.86 and 0.90, respectively.
Compulsive sexual behavior was assessed using the 13-item “Control” subscale of the Compulsive Sexual Behavior Inventory (Coleman et al., 2001). Each item was evaluated on a scale ranging from 1 = “Very frequently” to 5 = “Never.” A higher score indicates a lower degree of compulsiveness.
To explore the dimensionality of compulsive sexual behavior, a factor analysis was performed. Three separate dimensions of compulsive sexual behavior emerged from the analysis. The following four items loaded highest on Factor 1: “How often have you had trouble controlling your sexual urges,” “How often have you felt unable to control your sexual behavior,” “How often have you been unable to control your sexual feelings,” and “How often have you used sex to deal with worries or problems in your life?” Therefore, Factor 1 was called “Feelings and behavioral control.” The factor was saved as a new variable based on the factor scores (Cronbach’s alpha = 0.78).
The following four items loaded highest on Factor 2: “How often have you missed opportunities for productive and enhancing activities because of your sexual activity,” “How often have your sexual thoughts or behaviors interfered with the formation of friendships,” “How often have you developed excuses or reasons to justify your sexual behavior,” and “How often have your sexual activities caused financial problems for you?” Factor 2 was labeled as “Social consequences of compulsive sexual behavior.” The factor was saved as a new variable based on the factor scores (Cronbach’s alpha = 0.74).
The following five items loaded higher on Factor 3: “How often have you concealed or hidden your sexual behavior from others,” “How often have you felt guilty or shameful about aspects of your sexual behavior,” “How often have you felt emotionally distant when you were engaging in sex with others,” “How often have you had sex or masturbated more than you wanted to,” and “How often have you made pledges or promised to change or alter your sexual behavior?” Factor 3 was called “Shame over compulsive sexual behavior.” The factor was saved as a new variable based on the factor scores (Cronbach’s alpha = 0.70).
Statistical Analysis
All statistical analyses were performed using SPSS/PC version 24. For the purpose of the bivariate ANOVA analyses, the continuous psychological variables were recoded into new categorical variables with the alternatives low, medium, and high level. The cut point was set to get a similar number of respondents in each category. In order to predict the three dimensions of IH, hierarchical linear regression analyses were performed (Pallant, 2010). All observed differences with p-values at < 0.05 were considered as statistically significant.
Results
Table 2 shows mean scores on the three dimensions of IH by level of education, place of residence, and age. For the IH-dimensions “Personal comfort with gay identity” and “Social comfort with gay men,” there were no statistically significant differences in the reporting by the individual factors. There was a difference in the reporting on the IH dimension “Public identification as gay” by place of residence. MSM living in or around larger cities reported less IH than MSM who were residents in small towns (p < .01).

Table 3 shows the mean scores on three dimensions of IH by psychological factors. Only two psychological measures showed a statistically significant difference in the reporting between groups on “Public identification as gay”: shame over compulsive sexual behavior (p < .001) and sexual self-esteem (p < .01). For “Social comfort with gay men,” there was a statistically significant difference in the reporting by shame over compulsive sexual behavior (p < .01) and sexual satisfaction (p < .05). For the dimension “Personal comfort with gay identity,” there was a statistically significant difference in the reporting by NA status (p < .05), social consequences of compulsiveness (p < .05), and shame over compulsive sexual behavior (p < .001).


Table 4 shows the mean scores on the three dimensions of IH by social factors. The results showed the same pattern in the reporting for all dependent variables. MSM who were open about their sexual orientation had less IH than respondents who were closed (p < .001). Likewise, members of an LGBTQ organization had less IH than non-members (p < .001).
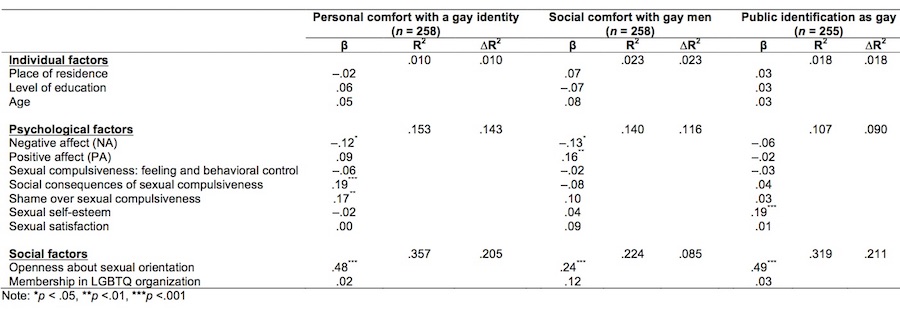
Hierarchical linear regression analyses were conducted to study the relationship between each of the IH dimensions and the selected predictors. The predictor variables were included in the analyses stepwise. First, the individual factors were inserted, followed by psychological factors, and lastly, the social factors were inserted in the model (Table 5). Only the results from the last regression analysis have been presented in Table 5, which means that the beta-values were controlled for to examine the effect of the other variables in the model.
As regards “Personal comfort with gay identity,” all the predictors included in the model explained 36% of the total variance. In the first step of the analysis of “Personal comfort with gay identity,” the individual factors contributed to explain 1% of the variance in the dependent variable (ΔR2), while the psychological factors explained another 14% of the variance in Step 2. In the last step, the social factors contributed to an increase of ΔR2 = 21%. The relative importance of the statistically significantly predictors appeared in the following descending order: openness about sexual orientation (β = 0.48), social consequences of compulsive sexual behavior (β = 0.19), shame over compulsive sexual behavior (β = 0.17), and negative affect (β = –0.12). This placement indicates that MSM who were open about their sexual orientation, who seldom experienced social consequences of or shame over compulsive sexual behavior, and who experienced little NA had less IH than their respective counterparts did.
The included predictors explained 22% of the total variance in “Social comfort with gay men.” In Step 1 of the analysis, the individual factors explained 2% (ΔR2) of the variance in the dependent variable. In Step 2, the psychological variables explained another 12% of the variance. And in Step 3, the social variables contributed with an increased variance of 9%. The relative importance of the statistically significant predictors was as follows: openness about sexual orientation (β = 0.24), positive affect (β = 0.16), and NA (β = –0.13). MSM who were open about their sexual orientation, and who experienced PA and had less NA, had less IH than their respective counterparts did.
The included independent variables explained 32% of the variance in “Public identification as gay.” The individual factors explained 2% of the variance in the dependent variable. In the next step, the psychological factors increased the explained variance by ΔR2 = 9%, and in the final step, the social factors contributed to an increase of ΔR2 = 21%. The relative importance of the statistically significant independent variables was as follows, in descending order: openness about sexual orientation (β = 0.49) and sexual self-esteem (β = 0.19). MSM who were open about their sexual orientation, who felt sexually self-secure, and who reported high sexual self-esteem had less IH than their respective counterparts did.
Discussion
To sum up, on controlling for the effect of psychological and social factors, we found no relationship between age, level of education, place of residence, and the three dimensions of IH. Openness about one’s sexual orientation was the best predictor for all IH dimensions. With regard to the IH dimension “Personal comfort with gay identity,” MSM who were open about their sexual orientation, who rarely experienced social consequences or shame over compulsive sexual behavior, and who had low NA exhibited a greater acceptance of their gay identity than others did. “Social comfort with gay men” was related to openness about one’s sexual orientation and PA. Respondents who were open about their sexual orientation and who experienced PA were more confident when socializing with gay men than others were. Finally, with respect to “Public identification as gay,” MSM who were open about their sexual orientation and who had higher sexual self-esteem scored higher than others did.

We found no relationship between the three dimensions of IH and individual factors. This was somewhat surprising since previous research has shown such relationships (David & Knight, 2008; Grossmann et al., 2001; Kuyper & Fokkema, 2010). One explanation for the discrepancy could be that the acceptance of homosexuality in Norwegian society is relatively high, particularly among those with higher education. Therefore, younger MSM in Norway may experience less stigma and fewer negative attitudes toward sexual minorities as compared to MSM in other countries. Furthermore, the one-third of respondents over 40 years of age may be biased, which means that that the non-significant relationship between age and IH may have occurred as a result of a selection bias. Additionally, the relationship between IH and place of residence was non-significant in the multivariate analyses. As Swank et al. (2012) pointed out, current place of residence need not necessarily reflect how much stigma a person has experienced in his life. Many young gay men grow up in small towns and move to the city to join the gay community. Later, when they are older and have established themselves financially and with a partner, they may move back home again.
We found that some of the psychological factors were associated with the three dimensions of IH. Low NA predicted less IH related to “Personal comfort with gay identity” and “Social comfort with gay men.” Furthermore, respondents who had high PA reported feeling more comfortable in the company of gay men as compared to men with low PA. This tendency indicates a relationship between affective status and IH. MSM with low negative affect most likely have developed an affective interpretation framework that provides better conditions to face prejudice and stigma from others. Those who feel satisfied with their life may have a more positive outlook on the future and feel enthusiastic and active (Norlander et al., 2002; Watson et al., 1988), which in turn makes them better prepared to face prejudice and stigma and thereby resist IH.
MSM who frequently experienced social consequences or shame owing to their compulsive sexual behavior were less confident with their own gay identity and had higher IH than others did. It is interesting that the lack of compulsive sexual behavior pertaining to emotional and behavioral control was not related to IH, but compulsive sexual behavior pertaining to social consequences and shame was. This inclination may indicate that for MSM who have internalized society’s stigma pertaining to their sexuality as something shameful and judgmental, the shame and social consequences aspects are of importance. Feelings of shame may prevent an individual from performing actions that would be perceived as deviating (Gazzaniga & Heatherton, 2003). Lastly, sexual self-esteem predicted IH related to public identification as gay. A high sexual self-esteem in MSM is likely to be associated with less negative emotions (Træen, Noor, Grey, Iantaffi et al., 2014) and with a reduced need for confirmation from others (Leary et al., 1999). Thus, MSM who have not been socialized to be ashamed of their sexuality are likely to have fewer negative thoughts related to their sexuality and therefore also less IH.
Openness about one’s sexual orientation correlated highly with a low degree of internalized homonegativity.
Limitations
Representativeness is a major challenge when it comes to research on sexual minorities. Participants in this study were recruited from a website for LGBTQ persons. As Swank et al. (2012) points out, this kind of data collection may provide a selection bias in the sense that not everyone has access to or uses the Internet, particularly older MSM. It may also underestimate MSM who are not “out.” Those who participated could have higher acceptance of their sexual orientation and be more involved in the LGBTQ community than those who did not use this website. Those who responded to the survey are therefore not necessarily representative of all MSM in Norway.
Conclusion
People who grow up in environments that are accepting of people of different sexual orientations are likely to internalize less homonegativity. This tendency bears importance for all who deviate from the heterosexual majority. It is therefore important to address acceptance of the diversity of sexual identities in sexual health promotion campaigns.
References
Bakkeli, V., & Elgvin, O. (2014). Kunnskapsoversikt om lesbiske, homofile, bifile og transpersoner [A review of knowledge about lesbian, homosexual, bisexual, and trans persons]. Fafo-notat, 1. Downloaded September 12, 2015 from http://www.fafo.no/images/pub/
Berg, R. C., Munthe-Kaas, H. M., & Ross, M. W. (2016). Internalized homonegativity: A systematic mapping review of empirical research. Journal of Homosexuality, 63(4), 541–558. doi:10.1080/00918369.2015.1083788
Coleman, E., Miner, M., Ohlerking, F., & Raymond, N. (2001). Compulsive sexual behavior inventory: A preliminary study of reliability and validity. Journal of Sex & Marital Therapy, 27, 325–332. doi:10.1080/009262301317081070
D’Augelli, A. R., Hershberger, S. L., & Pilkington, N. W. (1998). Lesbian, gay, and bisexual youth and their families: Disclosure of sexual orientation and its consequences. American Journal of Orthopsychiatry, 68, 361–371. doi:10.1037/h0080345
David, S., & Knight, B. G. (2008). Stress and coping among gay men: Age and ethnic differences. Psychology and Aging, 23(1), 62–69. doi:10.1037/0882-7974.23.1.62

Feinstein, B. A., Goldfried, M. R., & Davila, J. (2012). The relationship between experiences of discrimination and mental health among lesbians and gay men: An examination of internalized homonegativity and rejection sensitivity as potential mechanisms. Journal of Consulting and Clinical Psychology, 80(5), 917–927. doi:10.1037/a0029425
Finlayson, A. J. R., Sealy, J., & Martin, P. R. (2001). The differential diagnosis of problematic hypersexuality. Sexual Addiction & Compulsivity, 8(3/4), 241–251. doi:10.1080/107201601753459946
Finstad, L., & Høigård, C. (2006). Straff og Rett [Punishment and Justice]. Oslo: Pax Forlag.
Frost, D. M., & Meyer, I. H. (2009). Internalized homophobia and relationship quality among lesbians, gay men, and bisexuals. Journal of Counseling Psychology, 56, 97–109. doi:10.1037/a0012844
Gazzaniga, M. S., & Heatherton. T. F. (2003). Psychological Science: Mind, Brain, and Behavior. New York: W. W. Northon & Company.
Grossman, A. H., D’Augelli, A. R., & O’Connell, T. S. (2001). Being lesbian, gay, bisexual, and 60 or older in North America. Journal of Gay & Lesbian Social Services, 13, 23–40. doi:10.1300/J041v13n04_05
Herek, G. M. (1996). Heterosexism and homophobia. In R. P. Cabaj & T. S. Stein (Eds.), Textbook of Homosexuality and Mental Health (s.101–113). Washington, DC: American Psychiatric Press.
Herek, G. M. (2004). Beyond “homophobia”: Thinking about sexual prejudice and stigma in the twenty-first century. Sexuality Research & Social Policy, 1(2), 6–24. doi:10.1525/srsp.2004.1.2.6
Herek, G. M., Cogan, J. C., Gillis, J. R., & Glunt, E. K. (1998). Correlates of internalized homophobia in a community sample of lesbians and gay men. Journal of the Gay and Lesbian Medical Association, 2, 17–25.
Herek, G. M., Gillis, J. R., & Cogan, J. C. (2009). Internalized stigma among sexual minority adults: Insights from a social psychological perspective. Journal of Consulting Psychology, 56, 32–43. doi:10.1037/a0014672

Igartua, K. J., Gill, K., & Montoro, R. (2003). Internalized homophobia: A factor in depression, anxiety, and suicide in the gay and lesbian population. Canadian Journal of Community Mental Health, 22(2), 15–30. doi:10.7870/cjcmh-2003-0011
Kalichman, S. C., & Cain, D. (2004). The relationship between indicators of sexual compulsivity and high risk sexual practices among men and women receiving services from a sexually transmitted infection clinic. Journal of Sex Research, 41(3), 235–241. doi:10.1080/00224490409552231
Kuyper, L., & Fokkema, T. (2010). Loneliness among older lesbian, gay, and bisexual adults: The role of minority stress. Archives of Sexual Behavior, 39, 1171–1180. doi:10.1007/s10508-009-9513-7
Lambert, E. G., Ventura, L. A., Hall, D. E., & Cluse-Tolar, T. (2006). College students’ views on gay and lesbian issues. Journal of Homosexuality, 50(4), 1–30. doi:10.1300/J082v50n04_01
Leary, M., Tchividjian, L., & Kraxberger, B. (1999). Self-presentation can be hazardous to your health: Impression management and health risk. In R. F. Baumeister (Ed.), The Self in Social Psychology (p. 182–194). Philadelphia, PA: Psychology Press.
Malterud, K., & Anderssen, N. (2014). Helse blant lesbiske og bifile kvinner i Norge [Health among lesbians and bisexual women in Norway]. Bergen, Norway: Uni Research AS.
Mayfield, W. (2001). The development of an internalized homonegativity inventory for gay men. Journal of Homosexuality, 41, 53–76. doi:10.1300/J082v41n02_04
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129, 674−697. doi:10.1037/0033-2909.129.5.674
Moleiro, C., Pinto, N., & Freire, J. (2013). Effects of age on spiritual well-being and homonegativity: Religious identity and practices among LGB persons in Portugal. Journal of Religion, Spirituality, & Aging, 25(2), 93–111. doi:10.1080/15528030.2012.741561
Newcomb, M. E., & Mustanski, B. (2010). Internalized homophobia and internalizing mental health problems: A meta-analytic review. Clinical Psychology Review, 30, 1019–1029. doi:10.1016/j.cpr.2010.07.003

Norlander, T., Bood, S. Å., & Archer, T. (2002). Performance during stress: Affective personality, age, and regularity of physical exercise. Social Behavior and Personality, 30, 495–508. doi:10.2224/sbp.2002.30.5.495
Pachankis, J. E., Goldfried, M. R., & Ramrattan, M. E. (2008). Extension of the rejection sensitivity construct to the interpersonal functioning of gay men. Journal of Consulting and Clinical Psychology, 76(2), 306–317. doi:10.1037/0022-006X.76.2.306
Pallant, J. (2010). SPSS Survival Manual: A Step by Step Guide to Analysis Using SPSS. 4th Ed. Maidenhead: McGraw-Hill.
Paul, J. P., Catania, J., Pollack, L., Moskowitz, J., Canchola, J., Mills T., Binson, D., & Stall, R. (2002). Suicide attempts among gay and bisexual men: Lifetime prevalence and antecedents. American Journal of Public Health, 92, 1338–1345. doi:10.2105/AJPH.92.8.1338
Prell, E., & Træen, B. (2018). Minority stress and mental health among bisexual and lesbian women in Norway. (Submitted.)
Ross, M. W., & Rosser, B. R. S. (1996). Measurement and correlates of internalized homophobia: A factor analytic study. Journal of Clinical Psychology, 52(1), 15–21. doi:10.1002/(SICI)1097-4679(199601)52:1<15::AID-JCLP2>3.0.CO;2-V
Ross, M. W., Smolenski, D. J., Kajubi, P., Mandel, J. S., McFarland, W., & Raymond, H. F. (2010). Measurement of internalized homonegativity in gay and bisexual men in Uganda: Cross-cultural properties of the Internalized Homonegativity Scale. Psychology, Health, and Medicine, 15, 159–165. doi:10.1080/13548500903527746
Rosser, B. R. S., Bockting, W. O., Ross, M. W., Miner, M. H., & Coleman, E. (2008). The relationship between homosexuality, internalized homonegativity, and mental health in men who have sex with men. Journal of Homosexuality, 55(2), 185–203. doi:10.1080/00918360802129394
Rosser, B. R. S., Smolenski, D., Erickson, D., Iantaffi, A., Brady, S. S., Grey, J. A., Hald, G. M., Horvath, K. J., Kilian, G., Træen, B., & Wilkerson, J. M. (2013). The effects of gay sexual explicit media on the HIV risk behavior of men who have sex with men. AIDS and Behavior, 17, 1488–1498. doi:10.1007/s10461-013-0454-8
Rüütel, K., Valk, A., & Lõhmus, L. (2017) Suicidality and associated factors among men who have sex with men in Estonia. Journal of Homosexuality, 64, 770–785. doi:10.1080/00918369.2016.1236578

Smolenski, D. J., Diamond, P., Ross, M. W., & Rosser, B. R. S. (2010). Revision, criterion validity, and multi-group assessment of the Reactions to Homosexuality Scale. Journal of Personality Assessment, 92, 568–576. doi:10.1080/00223891.2010.513300
Smolenski, D. J., Ross, M. W., Risser, J. M. H., & Rosser, B. R. S. (2009). Sexual compulsivity and high-risk sex among Latino men: The role of internalized homonegativity and gay organizations. AIDS Care, 21(1), 42–49. doi:10.1080/09540120802068803
Snell, W. E., Fisher, T. D., & Walters, A. S. (1993). The multidimensional sexuality questionnaire: An objective self-report measure of psychological tendencies associated with human sexuality. Annals of Sex Research, 6, 27–55. doi:10.1007/BF00849744
Solomon, D., McAbee, J., Åsberg, K., & McGee, A. (2015). Coming out and the potential for growth in sexual minorities: The role of social reactions and internalized homonegativity. Journal of Homosexuality, 62(11), 1512–1538. doi:10.1080/00918369.2015.1073032
Swank, E., Frost, D. M., & Fahs, B. (2012). Rural location and exposure to minority stress among sexual minorities in the United States. Psychology and Sexuality, 3, 226–243. doi:10.1080/19419899.2012.700026
Szymanski, D. M., & Gupta, A. (2009). Examining the relationship between multiple internalized oppressions and African American lesbians, gay, bisexual, and questioning persons’ self-esteem and psychological distress. Journal of Counseling Psychology, 56(1), 110–118. doi:10.1037/a0013317
Thompson, E. R. (2007). Development and validation of an internationally reliable short-form of the positive and negative affect scale (PANAS). Journal of Cross-Cultural Psychology, 38, 227–242. doi:10.1177/0022022106297301
Tozer, E. E., & Hayes, J. A. (2004). Why do individuals seek conversion therapy? The role of religiosity, internalized homonegativity, and identity development. The Counseling Psychologist, 32, 716–740. doi:10.1177/0011000004267563
Træen, B., Noor, S. W., Grey, J., Iantaffi, A., Rosser, B. R. S., & Hald, G. M. (2014). Sexually explicit media and sexual risk behavior in a sample of men who have sex with men in Norway. Sexuality and Culture, 18, 1038–1051. doi:10.1007/s12119-014-9238-1
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology, 54, 1063–1070. doi:10.1037/0022-3514.54.6.1063
