
There is no doubt that the comorbidity between personality disorder and substance use disorder overall is high. Numerous studies have demonstrated the frequent covariance between these two disorders (Cacciola, Alterman, Rutherford, McKay, & Mulvaney, 2001; Fenton et al., 2012; Hasin & Kilcoyne, 2012; McGlashan et al., 2000; Thomas, Melchert, & Banken, 1999; Trull, Jahng, Tomko, Wood, & Sher, 2010; Verheul, 2001). It has been debated whether it is PD in general or Cluster B specifically that drives the covariation. It has also been discussed if the covariance can be explained by overlapping criteria (e.g., impulsivity in borderline personality disorder (BPD) and antisocial PD).
For example, in one study of opiate use disorders in the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), 50% of respondents had a PD. When controlling for the general criteria for PD, borderline personality disorder became a clear predictor for SUD (Jahng et al., 2011). It has been suggested that the covariation between BPD and SUD are linked via impulsivity (Jahng et al., 2011; McGlashan et al., 2000). Among SUD patients, a median of 57% (range 35%–73%) had concurrent PD (Verheul, 2001), and among PD in the general population, the prevalence of comorbid SUD was 42% for alcohol and 19% for substance use (Trull et al., 2010).

In Scandinavian samples, the co-occurrence of SUD in PD in a population-based study was 46% (Toftdahl, Nordentoft, & Hjorthøj, 2016). For female patients with SUD, BPD is the most common personality disorder (Landheim, Bakken, & Vaglum, 2003). Cluster B personality traits have been found to be independent risk factors for developing SUD (Cohen, Chen, Crawford, Brook, & Gordon, 2007; Walter et al., 2009). BPD has been found as a significant risk factor for the persistence of SUD (Fenton et al., 2012), but remission of SUD in BPD in a 10-year study was also common (Zanarini et al., 2011). Treatment of patients with BPD/SUD has been described as difficult due to high dropout rates and to relational problems that make the process of establishing a therapeutic alliance challenging (Karterud, Arefjord, Andresen, & Pedersen, 2009).
For instance, Cluster B traits present a barrier in forming a therapeutic alliance with SUD patients and Cluster B traits have been found to provoke distanced and overwhelmed/disorganized countertransference in helpers (Betan, Heim, Conklin, & Westen, 2005; Olesek et al., 2016; Thylstrup & Hesse, 2008). Concurrent PD/SUD results in a more serious substance use disorder and more substance use–related problems (Vélez-Moreno et al., 2016). Risk for suicide attempts is higher for BPD patients with comorbid SUD compared to BPD or SUD patients alone (Darke, Williamson, Ross, Teesson, & Lynskey, 2004; Yen et al., 2003), although one study found no correlation between suicide attempts and baseline PD (Bakken & Vaglum, 2007). Risk for treatment attrition is higher for PD/SUD compared to SUD alone (Ball, Carroll, Canning-Ball, & Rounsaville, 2006; Brorson, Arnevik, Rand-Hendriksen, & Duckert, 2013; Cacciola et al., 2001). In addition, Cluster B traits and a PD diagnosis have been found to influence outcome negatively for SUD patients (Marlowe, Kirby, Festinger, Husband, & Platt, 1997; Thomas et al., 1999), although in one study PD had no influence on the outcome of SUD at a six-year follow-up (Landheim, Bakken, & Vaglum, 2006).
Thus, when BPD and SUD co-occur, the patients seem to be struggling even more than when each of these serious disorders occurs alone, and therapeutically there are many pitfalls. Patients with dual diagnoses are marginalized, often excluded from psychiatric treatments, and most likely need additional support (Toftdahl, Nordentoft, & Hjorthøj, 2016). Many have voiced the need for targeted treatments for this group of patients (Hesse & Fridell, 2009; Ravndal, Vaglum, & Lauritzen, 2005; Vélez-Moreno et al., 2016).
Concerning evidence for efficacy of psychotherapy for BPD/SUD, the latest review found 10 controlled studies on BPD/SUD patients (Lee, Cameron, & Jenner, 2015). The studies included four studies with dialectical behavioral therapy (DBT), three with dual focused schema therapy (DFST), and three with dynamic deconstructive psychotherapy (DDP). DBT and DDP showed some reduction in symptoms and substance use while DFST had minimal effect on outcome. The authors conclude that the evidence base for treatment of co-occurring BPD/SUD needs more research and that some preliminary evidence exists to date in benefit of DBT and DDP.
Mentalization-based treatment has shown great promise with BPD patients in various RCTs and naturalistic cohort studies, both within the original environment (Bateman & Fonagy, 2001, 2009; Rossouw & Fonagy, 2012) and from other independent institutions (Bales et al., 2014; Bales et al., 2012; Jørgensen et al., 2014; Kvarstein et al., 2015). In some studies (Bateman & Fonagy, 2009; Jørgensen et al., 2013), the difference between the control condition (structured clinical management, supportive group psychotherapy) and MBT has not been that large regarding outcome. However, the superiority of MBT has been demonstrated when the severity of PD is taken into consideration (Bateman & Fonagy, 2013).
To date, there is only one unpublished study from Stockholm on MBT for BPD/SUD. In this RCT, patients received 18 months of MBT or treatment as usual (TAU) within an outpatient addiction treatment clinic. Surprisingly, the MBT patients (N=24) did not differ from the control group (N = 22) with respect to outcome. There was one near significant finding (Mann-Whitney p = 0.06) that demonstrated the MBT group had no suicide attempts during treatment, versus four in the control group (Philips, 2016). However, we cannot know for sure that treatment in this study was MBT proper since adherence was low (Karterud & Bateman, 2010; Möller, Karlgren, Sandell, Falkenström, & Philips, 2016; Philips, 2016). Another study on MBT with severely impaired young BPD patients involved 79% with comorbid SUD. In this study, MBT showed improvement on several outcome measures, and effect sizes were large (Bales et al., 2012).
Thus, to date, we still do not know whether MBT is an efficient approach for BPD/SUD patients. It could be that the presence of SUD has some consequences for treatment that we still do not fully understand. We have tentative knowledge that BPD/SUD patients seem to improve after MBT, but we also have knowledge of the opposite: no improvement at all. Many have advocated the importance of tailoring treatments to these patients who are so severely disordered. Still, we have only preliminary evidence that specialized treatment (e.g., DBT) for this patient group is beneficial (Lee et al., 2015). Against this backdrop, we aimed to investigate in a pilot project if MBT, a specialized tailored treatment for BPD, is promising in the treatment of a group of severely disordered dual diagnosis patients with BPD/SUD. Furthermore, we strove to investigate the feasibility aspects of implementation, delivery by clinicians, and acceptability for patients in order to clarify whether a larger study could be recommended on this population and within this context.
Research questions
Does mentalization-based treatment have any positive effect on BPD/SUD patients’ substance use and personality disorder (primary outcome)? Does mentalization-based treatment have any positive effect on symptom distress and/or interpersonal and social functioning (secondary outcome)? Is MBT feasible as a treatment and for investigation in a larger study format in a general drug clinic on female patients with dual PD/SUD?
Material and Methods
Subjects
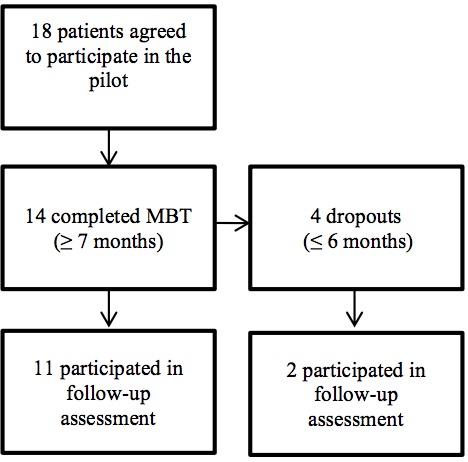
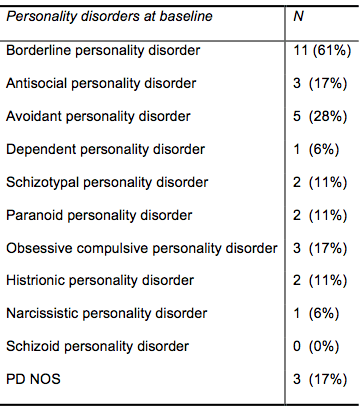
Patients were recruited from the inpatient and outpatient facilities of the Bergen Clinic Foundation (BCF). Patients in the BCF consist of both inpatients and outpatients with SUD, the majority with alcohol use disorder (40%–45%) and then equally distributed SUD diagnosis among cannabis, benzodiazepines and amphetamine dependency as most frequent. Multiple substance use is common; most patients have more than one SUD diagnosis. Most patients are without occupation (78%) and supported by different economic welfare benefits (75%–80%). A minority of the patients are female (27%) (Skutle, 2017). Because the BCF has an explicit focus on gender-specific treatment where males and females are given separate treatments, this pilot was performed with female patients alone. We went out broadly in the clinic asking for participants who were “difficult to treat,” female, and with a tentative diagnosis of BPD. Eighteen patients were included in the project. Inclusion criteria included being female and having a diagnosis of SUD together with a personality disorder with clinically significant borderline traits according to the SCID-II (Gibbon, Spitzer, & First, 1997). The full diagnosis of BPD was not necessary to enter the pilot. Exclusion criteria were diagnosis of schizophrenia and substitute opiate medication. See Table 2 for diagnostic profiles.
The patients were severely impaired, and all had histories of trauma. Seven of 18 had histories with rape, eight had been victims of violence in childhood, 10 had a history of neglect in childhood, and seven had experienced sexual trauma in childhood. Most patients had problems with violence and aggression. Ten of 18 had been violent toward people, 14 of 18 had been violent to material objects, and seven of 18 had been reported to the police for violent offences. Six patients had a prior history of psychotic episodes but not a diagnosis of schizophrenia. Their history of prior treatment was quite substantial, with a mean of four (range 1–15) prior admissions to inpatient treatment and a mean of three (range 1–7) periods of outpatient treatment.
They had a mean of two (range 1–4) SUD diagnoses and a mean of four (range 1–7) Axis I diagnoses at baseline. (See Table 2 for diagnostic characteristics.) All patients had maladaptive traits within the BPD category (range 3–9 traits). As for PD traits according to SCID-II, they had a mean of 18 (range 9–42) PD traits. The distribution of PDs can be seen in Table 3. Nine patients had more than one PD (range 2–5 PDs).
Clinical vignettes on one patient are hereby included to demonstrate a typical patient in this project:
Female patient, 28 years old, antisocial PD/BPD, polysubstance use disorder, and ADHD. History of neglect and conduct disorder in childhood. Before treatment, she uses amphetamine daily intravenously and in addition opiates and benzodiazepines. During assessment, she gets an ADHD diagnosis and starts on appropriate medication. Her level of functioning is very low, with a GAF score of 37. She has frequent impulsive, aggressive outbursts with people around her, both strangers and close relations. She gets easily agitated and sometimes uses violence or threats of violence. She is unemployed and receives welfare benefits. She finished two years of MBT. At follow-up she describes being abstinent from all drugs for the last four years. She has much fewer conflicts with others because she is able to see situations from the other’s perspective. She has started a part-time job and deals with the relational aspect of working by thinking things through instead of acting out on colleagues. She is very grateful for the treatment that helped her.
Patients were assessed prior to treatment, every six months during treatment, and at follow-up. The number of measurement points per patient varied with a mean of four (range 2–6). All patients were invited via post to participate in a follow-up assessment. They received a gift certificate of 500 NOK (60 Euro / 60 U.S. dollars) for participation. Thirteen patients participated. Five patients did not participate in the follow-up. Some descriptive data and length of treatment are included below. Their reasons for not participating in the follow-up were: 1) One patient threatened suicide if we ever contacted her again (13 months MBT); 2) one patient was of unknown whereabouts in another continent, and her family had no idea where and when she would be back (10 months MBT); 3) one patient angrily said no and hung up the telephone (six months MBT); 4) one patient agreed to come to follow-up but never showed up, and she never answered our requests again (one month MBT); 5) one patient was severely ill after a drug-related incident and was chronically hospitalized and unable to perform assessment (seven months MBT). Thus, compared to follow-up attenders, the mean duration of treatment was lower (seven vs. 22 months).
Follow-up assessments were performed at a mean of 22 (SD = 18) months after termination of MBT. In the follow-up, the pre-treatment battery was repeated together with qualitative interviews.


Dual focus mentalization-based treatment
All therapists were trained and experienced in the general treatment of SUD, which was delivered by the clinic. This training consisted of courses in motivational interviewing and basic courses on SUD. In addition, the psychologists had fulfilled or were enrolled in a five-year clinical specialization on drug addiction run by the Norwegian Psychological Association. Furthermore, all therapists and one social counselor were trained in MBT.
Training in MBT consisted of a three-day introductory course and a one-year specialization course (eight days). In addition, therapists received weekly video supervision with an expert in MBT and monthly video supervision with an external supervisor, also expert in MBT. Treatment was performed according to group and individual manuals (Karterud, 2011, 2012; Karterud & Bateman, 2010). Adherence was not measured, but weekly video supervision was conducted according to the manuals. Patients started out with 12 sessions of MBT psychoeducation and then continued with the group (MBT-G) and individual therapy (MBT-I). Maximal treatment duration was three years and involved weekly individual and group sessions throughout the entire period. Mean months in treatment were 22 (SD = 15). In dual focus MBT, focus on the mental function of SUD is of importance. Incidents of substance use are considered important and the focus is on exploring the mentalizing failure and interpersonal context prior to intake. All patients had access to a social counselor who was trained in MBT and who attended the supervisory sessions. The task of the social counselor was to offer help with social functioning in addition to increasing mentalization both there and then subsequently in encounters with the social welfare system, child protective services, and the like. The social counselor also did a thorough mapping of the patients’ social, economic, and work status and offered help with attaining their goals in social and work functioning.
Diagnostics
All therapists were trained in GAF and SCID-II assessments from a supervisor from the Norwegian Network of Personality-Focused Treatment Programs, and the assessment procedures were equal to those used by this network. (See for instance Kvarstein et al., 2015). Diagnostic reliability was not measured, but therapists were specially trained in the diagnostics of PD, and diagnoses were discussed thoroughly within the team and with the supervisor. In addition, according to the LEAD principle, diagnoses were open for adjustments during the clinical trajectory (Spitzer, 1983). At follow-up, diagnostics were performed by the first and fourth authors, who together evaluated SCID, GAF, and MINI diagnosis of all patients. Both also performed the diagnostic interviews.
Outcome measures
Axis I SUD diagnosis
Patients were interviewed with the Mini-International Neuropsychiatric Interview-Plus (M.I.N.I-Plus) before treatment and at follow-up (Sheehan et al., 1998). M.I.N.I-Plus is a structured diagnostic interview covering the most prevalent Axis I disorders within both DSM-IV and ICD-10.

Axis II disorders
Patients were diagnosed on Axis II by clinical interviews before treatment and at follow-up according to the Structured Clinical Interview for DSM-IV (SCID-II) (Gibbon et al., 1997). Following the LEAD principle, some of the diagnoses were revised after further clinical observation during the treatment period (Spitzer, 1983). The SCID-II is a semi-structured 94-item clinical interview that investigates the presence of PD according to the criteria from DSM-IV. Questions are answered with a yes or no and then further investigated through probing for examples. The interviewer decides if a patient fulfills criteria on SCID-II based on all available clinical information in addition to answers given during the interview.
SCL-90-R symptom distress
Symptoms were measured with SCL-90-R (Derogatis, 1977). The General Severity Index (GSI) is a well-known symptom distress measure and is widely used within clinical psychotherapy research. GSI gives a broad picture of a patient’s symptom distress in general. It is an average score of the total 90 items. The clinical/non-clinical cutoff level is set at GSI = 0.8 for women based on a Norwegian patient sample (Pedersen & Karterud, 2004). Cronbach’s alpha at baseline = 0.89.
Interpersonal functioning
Interpersonal functioning was measured as the Circumplex of Interpersonal Problems (CIP) (Pedersen, 2002), which is a Norwegian short version of the IIP-C (Horowitz, Rosenberg, Baer, Ureño, & Villaseñor, 1988). The mean sum score (CIP) correlates highly (r = 0.99) with the original IIP-C sum score (Pedersen, 2002). The clinical cutoff score of CIP is 0.8 (i.e., one standard deviation above mean IIP sum scores (M = 0.53) in a non-clinical Norwegian population) (Kvarstein et al., 2015; Pedersen, 2002). CIP has 48 items with a five-point scale, where subjects rate the degree of interpersonal problems. The CIP sum score is an indicator of the general level of experienced interpersonal problems and is based on a mean average of all 48 items. Cronbach’s alpha at baseline = 0.56.
Global assessment of functioning
The Global Assessment of Functioning (GAF) scale (Hall, 1995) is a widely used rating scale, ranging from 0 to 100, where 100 represents maximal global functioning (Pedersen & Karterud, 2012). GAF has shown high reliability between experienced judges and is a quick and easy instrument that can be used for measuring an individual patient’s need for treatment and at which level of health care (Pedersen, Hagtvet, & Karterud, 2007). A score of 60 indicates mild symptoms or impairment and is considered a good cutoff indicator for functional impairment in studies with treatment of PD (Kvarstein & Karterud, 2012).
Self-esteem
The Rosenberg Self-Esteem Scale (RSES) is a 10-item self-report questionnaire (Rosenberg, 1986). The 10 items are rated on a four-point scale from “strongly disagree” (1) to “strongly agree” (4). Cutoff for “normal” self-esteem lies at 3 (+/– 0.4). According to one study across 53 nations, RSES has good internal consistency with a mean Cronbach’s alpha coefficient reported of 0.81 (Schmitt & Allik, 2005). In the current study, Cronbach’s alpha at baseline was 0.89.
Work and social functioning scale
The Work and Social Adjustment Scale (WSAS) is a five-item self-report questionnaire (Mundt, Marks, Shear, & Greist, 2002). The five items are rated on an eight-point scale from “not impaired at all” to “severely impaired,” the responses to which are based on the last four weeks of functioning. The scoring range goes from 0 to 40, where a score above 20 represents severe psychopathology and functional impairment while a score between 10 and 20 represents functional impairment but less severe clinical symptomology. The cutoff score between clinical and non-clinical populations lies at 10. Cronbach’s alpha at baseline = 0.85.
Treatment retention
In this study, we defined dropout as less than or equal to six months of treatment, following the definition by Kvarstein and colleagues (2015) and the definition of “early dropouts” by Bateman & Fonagy (2009). In a study where the treatment duration is up to 36 months, we considered greater than six months to be a reasonable measure of dropout. Different MBT studies have varied in how they operationalize dropout from greater than three months (Laurenssen et al., 2013) to greater than two years (Jørgensen et al., 2013).
Statistical procedures
Linear mixed models (LMMs) were used for statistical analysis of the longitudinal data (Singer & Willett, 2003). For psychotherapy research, traditional data analytic techniques like Anova contain restrictive assumptions of sphericity (equal error variance across time points). They also utilize group means and variances and thus have several problems with handling missing data. Missing data have to be expected to some degree in naturalistic clinical settings, and if therapy is assumed to be efficient, larger variability at the start of the treatment is expected compared to the follow-up assessment (Tasca & Gallop, 2009). Thus, LMMs are tailored for psychotherapy research data in naturalistic settings, because doing so does not require data to meet the sphericity assumption. At the same time, it allows individuals to have different waves of data. The primary outcome data were measured at start of treatment and at follow-up (two timepoints); those were number of SCID-II PD traits, number of SCID-II borderline traits, and number of SUD diagnoses. The longitudinal secondary outcome data with 12 timepoints consisted of CIP, GAF, WSAS, GSI, and RSES. We performed a visual inspection of the data to determine whether a linear or nonlinear model best fitted the data and found that a linear model was a good fit. Time was modeled as a continuous variable with 6-month intervals and with baseline as time zero. Due to a low number of N, we allowed only random effects at baseline and kept the change over time as a fixed effect. Random effects at baseline imply that we allow the intercept to vary across individuals, and by keeping the slope as a fixed effect, we estimate the mean change over time across individuals. Due to a large amount of missing data across patients and measurement occasions, we imputed 20 data sets using the R package “mitml,” or “Tools for Multiple Imputation in Multilevel Modeling” (Grund, Robitzsch, & Lüdtke, 2017). We used the default inverse-Wishart priors, which give the minimum degrees of freedom with the largest dispersion. Furthermore, we used 50,000 burn-ins, 10,000 iterations apart. Estimates and standard errors were aggregated across the multiple imputed data sets (Barnard & Rubin, 1999), adjusting for smaller sample sizes using 28 degrees of freedom.
We calculated effect sizes’ pseudo R2 using the bivariate correlation between predicated scores and observed scores. We then transformed R2 to Cohen’s d through the formula d = 2r/√ (1 – r2) for pedagogical interpretative purposes. Analyses were performed with IBM 2015 SPSS statistics 23 and the R version 3.4.2 (2017, The R Foundation for Statistical Computing).
Patient consent
All patients received written information that explained the purpose of the study and allowed them to withdraw at any time. All the participants gave their written consent. The study was approved by the Regional Ethical Committee West (REK vest) for medical research in Norway.

Results
Primary outcome: Substance use and personality disorder
Axis I SUD diagnosis
At baseline, patients (N = 18) had a predicted mean of 1.78 (SE = 0.20) SUD diagnoses, and at follow-up, they had a predicted mean of 0.16 (SE = 0.19) SUD diagnoses. The change from pre-treatment to follow-up on SUD diagnosis was highly significant at the two-tailed level (t(28) = ‑6.26, p < .001). The effect size was very large (d = 2.12).
SCID-II personality traits
Prior to MBT, patients had a predicted mean of 17.72 (SE = 1.97) PD traits. At follow-up PD traits had declined to a predicted mean of 7.89 (SE = 1.83). The difference was highly significant at the two-tailed level (t(28) = ‑3.71, p = .001). The effect size was large (d = 1.31).
Borderline traits
At start of treatment, patients (N = 18) had a predicted mean of 5.39 (SE = 0.45) borderline traits according to the SCID-II interview. At follow-up the patients’ predicted mean of borderline traits had declined to 2.00 (SE = 0.43). The change from baseline to follow-up was highly significant at the two-tailed level (t(28) = ‑6.24, p < .001). The effect size was very large (d = 1.94). Only two out of 13 patients still fulfilled the criteria for BPD (five and six traits) at follow-up.
Secondary outcome measures
Symptom distress
At baseline, patients had a predicted mean GSI of 1.25 (SE = 0.14). Their GSI declined to a predicted mean of 0.57 (SE = 0.07) at follow-up. Change over time for GSI was significant (t(28) = ‑2.93, p = .028). The effect size was large (d = 1.18). The predicted mean change per six months was ‑0.06 (SE = 0.02). Nine out of 13 patients were below the clinical cutoff at follow-up assessment (GSI ≤ 0.8).
Interpersonal functioning
At baseline, the predicted mean of CIP was 1.28 (SE = 0.10). It decreased to a predicted mean of 0.90 (SE = 0.07) at follow-up. Effect size for change over time in CIP was moderate (d = 0.71) and change from baseline to follow-up was near significant (t(28) = ‑2.26, p = .073). The predicted mean change per six months was ‑0.03 (SE = 0.02). Concerning the clinical cutoff (0.8), six out of 13 patients were below or equal to that at follow-up assessment (CIP ≤ 0.8).
Global assessment of functioning
At baseline, patients had a predicted mean of GAF at 46.89 (SE = 2.15). At follow-up, their predicted GAF score had increased to 67.81 (SE = 1.00). Change over time for GAF was significant (t(28) = 4.64, p = .004) and the change rate per six months was 1.90 (SE = 0.41). The effect size was large (d = 2.06). Looking at the clinical cutoff with a GAF score above the level of 60, 10 out of 13 patients were assessed to be higher or equal to 60 at follow-up.
Self-esteem
RSES at start of treatment had a predicted mean of 2.34 (SE = 0.15). This figure increased to a predicted mean of 3.06 (SE = 0.10) at follow-up. Change over time for RSES was significant (t(28) = 3.34, p = .012) and the change rate per six months was 0.07 (SE = 0.02). The effect size for change until follow-up was large (d = 0.96). Looking at the clinical cutoff, defined as ranging from 2.6 to 3.4, only three patients were within the range of normal self-esteem at follow-up. Eight patients scored lower than the lower cutoff of 2.6, and two patients scored higher than the upper cutoff of 3.4.
Work functioning
WSAS at start of treatment had a predicted mean of 18.71 (SE = 1.74), and at follow-up the predicted mean of WSAS had dropped to 3.79 (SE = 0.73). For WSAS, the change over 5.5 years was also highly significant (t(28) = ‑4.13, p =.006) and the change rate per six months was ‑1.36 (SE = 0.33). The effect size for change until follow-up was large (d = 1.87). In WSAS, the cutoff score between clinical and non-clinical populations lies at 10, and nine out of 13 patients were equal to or below that cutoff score. The remaining four patients were all within the range of 10–20, suggesting functional impairment but less severe clinical symptomology.


Treatment retention
Four out of 18 patients (22%) were defined as dropouts (≤ six months in therapy). Five patients did not attend to the follow-up assessment for various reasons, which included saying no, being unavailable, discontentment with therapists, avoiding the appointments, serious injured to one patient after a drug-related accident.
Discussion
The aim of the present study was to investigate whether patients with BPD/SUD could benefit from participating in a specialized treatment, MBT, developed for patients with BPD. Our research questions were: 1) did participants improve on substance use disorder and 2) did they enter a positive trajectory regarding their BPD? Furthermore, we wanted to investigate participants’ improvements on secondary outcome measures: interpersonal functioning, global functioning, social functioning, and symptom severity. The main findings of our study were that patients with BPD/SUD showed significant improvement on both primary and secondary outcome measures. Effect sizes ranged from moderate to very large, with most being large.

Substance use decline
This MBT pilot was tailored to deal with the comorbidity of BPD/SUD since the trial happened within a specialized clinic for substance use disorders and all therapists were trained in the treatment of substance use disorder and personality disorder. Thus, a dual focus on both core issues of PD together with a continuous focus on substance use and how to reduce it were imminent during the whole treatment trajectory. Therapists probably also tolerated better (dealt with their countertransference), because of their experience and training, the hardcore realities of patients living in the peripheral life situations of drug and alcohol addiction.
The use of an MBT-oriented social counselor and the focus both psycho-pedagogically and therapeutically on substance use and its relation to mentalizing are somewhat different from how MBT is delivered in other settings. For example, the specific focus on exploring mentalizing failure prior to substance intake is an intervention that needs to be utilized when working with BPD/SUD patients. Our pilot also offered 36 months of treatment as opposed to the original authors who suggest 18 to 24 months (Bateman & Fonagy, 2016). The present study is performed as a pilot, and we had no randomization or control group. Conclusions must be taken with great care. Still, we found our results regarding SUD intriguing.
To our surprise, many of the patients achieved full remission of their SUD. Several of them had long histories with outpatient and inpatient treatment in our own institution and thus were in danger of being viewed upon as chronic patients. We believe that the model of primacy of PD in the etiology of PD/SUD is of interest (Vélez-Moreno et al., 2016; Verheul & van den Brink, 2005). In this pilot, the focus was on increasing patients’ ability to mentalize (an issue related to their PD symptomology), especially during moments of emotional activation and attachment-related arousal. In MBT, this focus is systematic and continues throughout the whole clinical trajectory.
It seems that by targeting BPD-related problems, there is an effect on SUD for these patients. Other inpatient and outpatient treatments had not achieved these results before. In some studies on Nordic SUD patients (with high prevalence of PD), the remission of SUD at five- and six-year follow-up after treatment is not that encouraging, with relapse rates at 70% (Landheim et al., 2006) and 54% (Fridell & Hesse, 2006). We performed a two-year follow-up and thus cannot directly compare our findings to the studies above. In another longitudinal study, disappearance of BPD coincided with the disappearance of SUD (Paris & Zweig-Frank, 2001). This tendency converges with our findings where SUD and BPD both demonstrated substantial decline from baseline to follow-up. It also supports the notion that by focusing on BPD-related difficulties through increasing the ability of mentalizing (Philips et al., 2012), there is a possible effect on SUD as well (Outcalt et al., 2016). But there are some who have advocated that SUD must be seen as a chronic disorder and that treatment needs to shift focus from curing the disorder to symptom relief (McLellan, 2002). Our findings contradict this perspective and give a tentatively more positive view on SUD (and comorbid PD). There is perhaps a possibility of treating both disorders, given targeted treatments.
Reduction of borderline symptomology
MBT is a tailored treatment for BPD (Bateman & Fonagy, 2016), and assessing whether patients still have BPD after completion of treatment is thus important. In our study, both the number of personality disorder criteria declined, and the diagnosis of BPD disappeared at follow-up. This is quite encouraging with respect to the efficiency of MBT with this dual diagnosis patient group, and it supports the notion that MBT is increasingly efficient in line with the severity of the patient group pathology (Bateman & Fonagy, 2013). Two patients still fulfilled the criteria for BPD at follow-up. These patients deserve detailed case studies. The decline in both borderline personality disorder and substance use disorder during the same clinical trajectory supports the notion that PD and SUD are connected and causally connected to each other in some way. Three models have been proposed on the interconnectedness of PD/SUD, and most support lies with the model where PD is primary to SUD (Verheul & van den Brink, 2005).
Improvement in social functioning, self-esteem, and symptomatic distress
Overall the results on our secondary outcome measures demonstrate improvement. For all our outcome measures except for interpersonal functioning, the predicted trajectories lie within the non-clinical domain at follow-up. On self-esteem, symptom distress, general functioning, and work and social functioning, patients reach non-clinical levels. These results are quite encouraging. Interpersonal functioning does significantly change from baseline to follow-up but does not at any point reach non-clinical levels. Treating dual diagnosis patients with comorbid personality disorder is challenging. We are just getting started in gaining enough knowledge on what these patients need for positive change trajectories. Many of our patients in this pilot reached symptomatic improvement and remission of SUD and PD. Further follow-up studies need to be performed to investigate if these changes endure in the longitudinal trajectory of MBT patients.
Do BPD/SUD patients have unique trajectories regarding GSI and CIP?
Do they get worse before they get better? Our sample of dual diagnosis patients reported lower symptom distress on the GSI at baseline than patients with BPD alone; see for instance Bateman & Fonagy (2009), Kvarstein et al. (2015), and Laurenssen et al. (2013). GSI in these studies were respectively 2.0, 2.1, and 2.2 versus our sample who reported predicted baseline levels of GSI to be 1.3. The one MBT study that had a sample of BPD patients where 79% had comorbid SUD also demonstrated their baseline symptom distress scores to be somewhat lower than the studies above, at 1.7 (Bales et al., 2012).
The patients in our sample also had lower CIP sum scores on baseline (1.3) than other studies with borderline personality disorder (2.0, 1.7) (Bateman & Fonagy, 2009; Kvarstein et al., 2015). We think this tendency demonstrates how SUD intervenes with the subjective experience of interpersonal problems and symptom distress. Substance use has been suggested to function as a regulator of emotional activation, particularly during moments of an activated attachment system (Philips et al., 2012). This hypothesis converges with theories in the field where substance use has been suggested to potently interfere with attachment needs (Cihan, Winstead, Laulis, & Feit, 2014; Insel, 2003). This gives indices that the psychotherapeutic trajectory for BPD/SUD patients could possibly involve a worsening of the subjective experience of symptom severity and interpersonal functioning when and if their substance use declines. These nonlinear change trajectories were not possible to model in this study due to a low number of n.
The reasons for these discrepancies between BPD/SUD patients and BPD alone are unknown and require further empirical investigation. We speculate the following: 1) substance use has an effect on the subjective experience of symptom distress and interpersonal functioning and 2) BPD/SUD patients have unique trajectories during psychotherapy on symptom distress and interpersonal functioning.
Further studies are needed to investigate these hypotheses on the uniqueness of BPD/SUD trajectories of change in psychotherapy.

Treatment retention
Dropout in the treatment of BPD/SUD group of patients is a common problem (Ball et al., 2006; Brorson et al., 2013). Therapeutic alliance can be a challenge for SUD patients with Cluster B traits (Olesek et al., 2016). Defining dropout as equal to or less than six months of treatment, we had in our study four out of 18 patients dropping out (22%). Our dropout rate is lower than numbers reported from other studies with dual diagnosis patients. In dual diagnosis DBT studies, the dropout rates have ranged from 36% to 55% (Axelrod, Perepletchikova, Holtzman, & Sinha, 2011; Linehan et al., 2002; Linehan et al., 1999). In MBT studies with BPD alone, the dropout rate has varied from 5% to 43% (Jørgensen et al., 2013; Kvarstein et al., 2015).
The problem is that the respective studies above do not define dropout equally. Our dropout definition is equivalent to Kvarstein and colleagues (2015) (5%), and it seems that compared with them, our dropout rate is too high. Nevertheless, a dropout rate of 22% is acceptable with a patient group known for problems with alliance and treatment retention. We suggest, however, that further empirical investigations would shed light on the reasons for dropout in this patient group, so that we could better tailor our treatment programs.
Strength and limitations
There are several problems with this study, which implies that the conclusions should be taken with great care. First, the study did not involve any control group or randomization. Thus, we cannot conclude that the changes these patients underwent were caused by the actual treatment. In the natural trajectory of BPD patients, symptomatic and personality distress does improve with the passage of time (Gunderson et al., 2011; Zanarini, Frankenburg, Hennen, & Silk, 2003). However, these patients’ social functioning is less amenable to improvement and the prognosis is worse when combined with SUD (Fridell & Hesse, 2006; Walter et al., 2009).
Second, the number of patients was very small, as is often a problem in treatment studies of BPD/SUD patients. The statistical analyses were limited by the small n, and the only analyses we could perform were to substantiate that changes had occurred. Nonlinear change trajectories could not be investigated, and comparisons between different subgroups in the sample were not possible (e.g., dropouts vs. treated patients).
Third, we did not have any endpoint data on five patients. A full data set might have influenced the results in a negative manner. The response of some participants to our request might indicate that they still have significant personality problems. The duration of their treatments was also lower than our follow-up completers. We would also like to mention that supervisors and trainers from the Norwegian Institute of Mentalizing were involved, which could generate a positive bias. However, the most obvious contribution of these trainers and supervisors was to secure adherence to and the quality of the treatment that was delivered.
The favorable results of this pilot study call for a larger randomized study.
A considerable strength of the study was its ecological validity (i.e., that it was conducted in a clinical naturalistic setting). It is also noteworthy that all patients had multiple experiences with former treatments, both inpatient and outpatient treatments, and most of them from the same clinic where this pilot was performed. Earlier treatment had not had any lasting effect on their personality disorder or SUD.
Conclusion
Patients suffering from both severe personality disorder of the borderline type and substance abuse are known to be difficult to treat and have a very poor prognosis. Our study indicates that MBT might be a promising treatment modality for this comorbid condition. We found that for the majority of the patients, their drug and alcohol consumption and personality problems improved considerably. However, the results for the cohort as a whole are somewhat uncertain since 28% of the patients did not respond to follow-up. Furthermore, because this was a feasibility study, our findings indicate that MBT is implementable in a drug clinic, that clinicians and patients find the treatment protocol acceptable, and that data can be routinely collected. These favorable results indeed call for a larger randomized study.
References
Axelrod, S. R., Perepletchikova, F., Holtzman, K., & Sinha, R. (2011). Emotion regulation and substance use frequency in women with substance dependence and borderline personality disorder receiving dialectical behavior therapy. The American Journal of Drug and Alcohol Abuse, 37, 37–42. doi:10.3109/00952990.2010.535582
Bakken, K., & Vaglum, P. (2007). Predictors of suicide attempters in substance-dependent patients: A six-year prospective follow-up. Clinical Practice and Epidemiology in Mental Health, 3(1), 20. doi:10.1186/1745-0179-3-20
Bales, D. L., Timman, R., Andrea, H., Busschbach, J. J., Verheul, R., & Kamphuis, J. H. (2014). Effectiveness of day hospital mentalization‐based treatment for patients with severe borderline personality disorder: A matched control study. Clinical Psychology & Psychotherapy, 22(5), 409–417. doi:10.1002/cpp.1914

Bales, D. L., van Beek, N., Smits, M., Willemsen, S., Busschbach, J. J., Verheul, R., & Andrea, H. (2012). Treatment outcome of 18-month, day hospital mentalization-based treatment (MBT) in patients with severe borderline personality disorder in the Netherlands. Journal of Personality Disorders, 26(4), 568–582. doi:10.1521/pedi.2012.26.4.568
Ball, S. A., Carroll, K. M., Canning-Ball, M., & Rounsaville, B. J. (2006). Reasons for dropout from drug abuse treatment: Symptoms, personality, and motivation. Addictive Behaviors, 31(2), 320–330. doi:10.1016/j.addbeh.2005.05.013
Barnard, J., & Rubin, D.B. (1999). Small sample degrees of freedom with multiple imputation. Biometrica, 86, 948–955. doi:10.1093/biomet/86.4.948
Bateman, A., & Fonagy, P. (2001). Treatment of borderline personality disorder with psychoanalytically oriented partial hospitalization: An 18-month follow-up. American Journal of Psychiatry, 158(1), 36–42. doi:10.1176/appi.ajp.158.1.36
Bateman, A., & Fonagy, P. (2009). Randomized control trial of outpatient mentalization-based treatment vs. structured clinical management for borderline personality disorder. American Journal of Psychiatry, 166(12), 1355–1364. doi:10.1176/appi.ajp.2009.09040539
Bateman, A., & Fonagy, P. (2013). Impact of clinical severity on outcomes of mentalisation-based treatment for borderline personality disorder. The British Journal of Psychiatry, 203, 221–227. doi:10.1192/bjp.bp.112.121129
Bateman, A., & Fonagy, P. (2016). Mentalization-based treatment for personality disorders: A practical guide. New York: Oxford University Press. doi:10.1093/med:psych/9780199680375.001.0001
Betan, E., Heim, A. K., Zittel Conklin, C., & Westen, D. (2005). Countertransference phenomena and personality pathology in clinical practice: An empirical investigation. American Journal of Psychiatry, 162(5), 890–898. doi:10.1176/appi.ajp.162.5.890
Brorson, H. H., Arnevik, E. A., Rand-Hendriksen, K., & Duckert, F. (2013). Drop-out from addiction treatment: A systematic review of risk factors. Clinical Psychology Review, 33(8), 1010–1024. doi:10.1016/j.cpr.2013.07.007
Cacciola, J. S., Alterman, A. I., Rutherford, M. J., McKay, J. R., & Mulvaney, F. D. (2001). The relationship of psychiatric comorbidity to treatment outcomes in methadone maintained patients. Drug and Alcohol Dependence, 61(3), 271–280. doi:10.1016/S0376-8716(00)00148-4

Cihan, A., Winstead, D. A., Laulis, J., & Feit, M. D. (2014). Attachment theory and substance abuse: Etiological links. Journal of Human Behavior in the Social Environment, 24(5), 531–537. doi:10.1080/10911359.2014.908592
Cohen, P., Chen, H., Crawford, T. N., Brook, J. S., & Gordon, K. (2007). Personality disorders in early adolescence and the development of later substance use disorders in the general population. Drug and Alcohol Dependence, 88(S1), S71–S84. doi:10.1016/j.drugalcdep.2006.12.012
Darke, S., Williamson, A., Ross, J., Teesson, M., & Lynskey, M. (2004). Borderline personality disorder, antisocial personality disorder, and risk-taking among heroin users: Findings from the Australian Treatment Outcome Study (ATOS). Drug and Alcohol Dependence, 74(1), 77–83. doi:10.1016/j.drugalcdep.2003.12.002
Derogatis, L.R. (1977). SCL-90. Administration, Scoring, and Procedures Manual-I for the R (revised) Version and Other Instruments of the Psychopathology Rating Scales Series. Chicago: Johns Hopkins University School of Medicine.
Fenton, M. C., Keyes, K., Geier, T., Greenstein, E., Skodol, A. E., Krueger, B., . . . Deborah, H. S. (2012). Psychiatric comorbidity and the persistence of drug use disorders in the United States. Addiction, 107(3), 599–609. doi:10.1111/j.1360-0443.2011.03638.x
Fridell, M., & Hesse, M. (2006). Psychiatric severity and mortality in substance abusers: A 15-year follow-up of drug users. Addictive Behaviors, 31(4), 559–565. doi:10.1016/j.addbeh.2005.05.036
Gibbon, M., Spitzer, R. L., & First, M. B. (1997). User’s Guide for the Structured Clinical Interview for DSM-IV Axis II Personality Disorders: SCID-II. Arlington, VA: American Psychiatric Publishing
Grund, S., Robitzsch, A., & Luedtke,.O (2017, March 3). Mitml: Tools for Multiple Imputation in Multilevel Modeling. R package version 0.3-5. Retrieved from https://CRAN.R-project.org/package=mitml
Gunderson, J. G., Stout, R. L., McGlashan, T. H., Shea, M. T., Morey, L. C., Grilo, C. M., . . . Skodol, A. E. (2011). Ten-year course of borderline personality disorder. Archives of General Psychiatry, 68(8), 827–837. doi:10.1001/archgenpsychiatry.2011.37
Hall, R. C. (1995). Global assessment of functioning: A modified scale. Psychosomatics, 36(3), 267–275. doi:10.1016/S0033-3182(95)71666-8

Hasin, D., & Kilcoyne, B. (2012). Comorbidity of psychiatric and substance use disorders in the United States: Current issues and findings from the NESARC. Current Opinion in Psychiatry, 25(3), 165. doi:10.1097/YCO.0b013e3283523dcc
Hesse, M., & Fridell, M. (2009). Treating the patient with comorbidity. Evidence-Based Addiction Treatment, 327, 327–343. doi:10.1016/B978-0-12-374348-0.00017-3
Horowitz, L. M., Rosenberg, S. E., Baer, B. A., Ureño, G., & Villaseñor, V. S. (1988). Inventory of interpersonal problems: Psychometric properties and clinical applications. Journal of Consulting and Clinical Psychology, 56(6), 885. doi:10.1037/0022-006X.56.6.885
IBM (2015). IBM SPSS Statistics for Windows, version 23.0.
Insel, T. R. (2003). Is social attachment an addictive disorder? Physiology & Behavior, 79(3), 351–357. doi:10.1016/S0031-9384(03)00148-3
Jahng, S., Trull, T. J., Wood, P. K., Tragesser, S. L., Tomko, R., Grant, J. D., . . . Sher, K. J. (2011). Distinguishing general and specific personality disorder features and implications for substance dependence comorbidity. Journal of Abnormal Psychology, 120(3), 656. doi:10.1037/a0023539
Jørgensen, C. R., Bøye, R., Andersen, D., Blaabjerg, A. H. D., Freund, C., Jordet, H., & Kjølbye, M. (2014). Eighteen months post-treatment naturalistic follow-up study of mentalization-based therapy and supportive group treatment of borderline personality disorder: Clinical outcomes and functioning. Nordic Psychology, 66(4), 254–273. doi:10.1080/19012276.2014.963649
Jørgensen, C. R., Freund, C., Bøye, R., Jordet, H., Andersen, D., & Kjølbye, M. (2013). Outcome of mentalization‐based and supportive psychotherapy in patients with borderline personality disorder: A randomized trial. Acta Psychiatrica Scandinavica, 127(4), 305–317. doi:10.1111/j.1600-0447.2012.01923.x
Karterud, S. (2011). Manual for Mentaliseringsbasert Psykoedukativ Gruppeterapi (MBT-I). Oslo: Gyldendal Akademisk.
Karterud, S. (2012). Manual for Mentaliseringsbasert Gruppeterapi (MBT-G). Oslo: Gyldendal Akademisk.
Karterud, S., Arefjord, N., Andresen, N. E., & Pedersen, G. (2009). Substance use disorders among personality disordered patients admitted for day hospital treatment: Implications for service developments. Nordic Journal of Psychiatry, 63(1), 57–63. doi:10.1080/08039480802298705
Karterud, S., & Bateman, A. (2010). Manual for Mentaliseringsbasert Terapi (MBT) og MBT Vurderingsskala: Versjon Individualterapi. Oslo: Gyldendal Akademisk.
Kvarstein, E. H., & Karterud, S. (2012). Large variations of global functioning over five years in treated patients with personality traits and disorders. Journal of Personality Disorders, 26(2), 141. doi:10.1521/pedi.2012.26.2.141
Kvarstein, E. H., Pedersen, G., Urnes, Ø., Hummelen, B., Wilberg, T., & Karterud, S. (2015). Changing from a traditional psychodynamic treatment program to mentalization‐based treatment for patients with borderline personality disorder: Does it make a difference? Psychology and Psychotherapy: Theory, Research, and Practice, 88(1), 71–86. doi:10.1111/papt.12036
Landheim, A., Bakken, K., & Vaglum, P. (2003). Gender differences in the prevalence of symptom disorders and personality disorders among poly-substance abusers and pure alcoholics. European Addiction Research, 9(1), 8–17. doi:10.1159/000067732
Landheim, A. S., Bakken, K., & Vaglum, P. (2006). Impact of comorbid psychiatric disorders on the outcome of substance abusers: A six-year prospective follow-up in two Norwegian counties. BMC Psychiatry, 6(1), 44. doi:10.1186/1471-244X-6–44
Laurenssen, E. M. P., Hutsebaut, J., Feenstra, D. J., Bales, D. L., Noom, M. J., Busschbach, J. J. V., . . . Luyten, P. (2013). Feasibility of mentalization-based treatment for adolescents with borderline symptoms: A pilot study. Psychotherapy, 51(1), 159–166. doi:10.1037/a0033513
Lee, N. K., Cameron, J., & Jenner, L. (2015). A systematic review of interventions for co‐occurring substance use and borderline personality disorders. Drug and Alcohol Review, 34(6), 663–672. doi:10.1111/dar.12267
Linehan, M. M., Dimeff, L. A., Reynolds, S. K., Comtois, K. A., Welch, S. S., Heagerty, P., & Kivlahan, D. R. (2002). Dialectical behavior therapy versus comprehensive validation therapy plus 12-step for the treatment of opioid-dependent women meeting criteria for borderline personality disorder. Drug and Alcohol Dependence|, 67, 13–26. doi:10.1016/S0376-8716(02)00011-X
Linehan, M. M., Schmidt, H., Dimeff, L. A., Craft, J. C., Kanter, J., & Comtois, K. A. (1999). Dialectical behavior therapy for patients with borderline personality disorder and drug‐dependence. The American Journal on Addictions, 8(4), 279–292. doi:10.1080/105504999305686

Marlowe, D. B., Kirby, K. C., Festinger, D. S., Husband, S. D., & Platt, J. J. (1997). Impact of comorbid personality disorders and personality disorder symptoms on outcomes of behavioral treatment for cocaine dependence. The Journal of Nervous and Mental Disease, 185(8), 483–490. doi:10.1097/00005053-199708000-00002
McGlashan, T. H., Grilo, C. M., Skodol, A. E., Gunderson, J. G., Shea, M. T., Morey, L. C., . . . Stout, R. L. (2000). The collaborative longitudinal personality disorders study: baseline Axis I/II and II/II diagnostic co‐occurrence. Acta Psychiatrica Scandinavica, 102(4), 256–264. doi:10.1034/j.1600-0447.2000.102004256.x
McLellan, A. T. (2002). Have we evaluated addiction treatment correctly? Implications from a chronic care perspective. Addiction, 97(3), 249–252. doi:10.1046/j.1360-0443.2002.00127.x
Mundt, J. C., Marks, I. M., Shear, M. K., & Greist, J. M. (2002). The work and social adjustment scale: A simple measure of impairment in functioning. The British Journal of Psychiatry, 180(5), 461–464. doi:10.1192/bjp.180.5.461
Möller, C., Karlgren, L., Sandell, A., Falkenström, F., & Philips, B. (2016). Mentalization-based therapy adherence and competence stimulates in-session mentalization in psychotherapy for borderline personality disorder with comorbid substance dependence. Psychotherapy Research, 27(6), 1–17. doi:10.1080/10503307.2016.1158433
Olesek, K. L., Outcalt, J., Dimaggio, G., Popolo, R., George, S., & Lysaker, P. H. (2016). Cluster B personality disorder traits as a predictor of therapeutic alliance over time in residential treatment for substance use disorders. The Journal of Nervous and Mental Disease, 204(10), 736–740. doi:10.1097/NMD.0000000000000553
Outcalt, J., Dimaggio, G., Popolo, R., Buck, K., Chaudoin-Patzoldt, K. A., Kukla, M., . . . Lysaker, P. H. (2016). Metacognition moderates the relationship of disturbances in attachment with severity of borderline personality disorder among persons in treatment of substance use disorders. Comprehensive Psychiatry, 64, 22‒28. doi:10.1016/j.comppsych.2015.10.002
Paris, J., & Zweig-Frank, H. (2001). A 27-year follow-up of patients with borderline personality disorder. Comprehensive Psychiatry, 42(6), 482–487. doi:10.1053/comp.2001.26271
Pedersen, G. (2002). Norsk revidert versjon av Inventory of Interpersonal Problems-Circumplex (IIP-C). Tidsskrift for Norsk Psykologforening, 39(1), 25–34.
Pedersen, G., Hagtvet, K. A., & Karterud, S. (2007). Generalizability studies of the Global Assessment of Functioning: Split version. Comprehensive Psychiatry, 48(1), 88–94. doi:10.1016/j.comppsych.2006.03.008

Pedersen, G., & Karterud, S. (2004). Is SCL‐90R helpful for the clinician in assessing DSM‐IV symptom disorders? Acta Psychiatrica Scandinavica, 110(3), 215–224. doi:10.1111/j.1600-0447.2004.00321.x
Pedersen, G., & Karterud, S. (2012). The symptom and function dimensions of the Global Assessment of Functioning (GAF) scale. Comprehensive Psychiatry, 53(3), 292–298. doi:10.1016/j.comppsych.2011.04.007
Philips, B. (2016). Passar MBT för patienter med dubbeldiagnos? Paper presented at the Nordisk mentaliseringskonferens 2016, Stockholm.
Philips, B., Kahn, U., & Bateman, A. (2012). Drug Addiction. In A. Bateman & P. Fonagy (Eds.), Handbook of Mentalizing in Mental Health Practice. London: American Psychiatric Publishing.
Ravndal, E., Vaglum, P., & Lauritzen, G. (2005). Completion of long-term inpatient treatment of drug abusers: A prospective study from 13 different units. European Addiction Research, 11(4), 180–185. doi:10.1159/000086399
R version 3.4.2 (2017). The R Foundation for Statistical Computing.
Rosenberg, M. (1986). Conceiving the Self. Malabar, FL:∂ RE Krieger.
Rossouw, T. L., & Fonagy, P. (2012). Mentalization-based treatment for self-harm in adolescents: A randomized controlled trial. Journal of the American Academy of Child and Adolescent Psychiatry, 51(12), 1304–1313. doi:10.1016/j.jaac.2012.09.018
Schmitt, D. P., & Allik, J. (2005). Simultaneous administration of the Rosenberg Self-Esteem Scale in 53 nations: Exploring the universal and culture-specific features of global self-esteem. Journal of Personality and Social Psychology, 89(4), 623. doi:10.1037/0022-3514.89.4.623
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., . . . Dunbar, G. C. (1998). The Mini-International Neuropsychiatric Interview (MINI): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. Journal of Clinical Psychiatry, 59(S20), 22–33.

Singer, J. D., & Willett, J. B. (2003). Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence: Oxford University Press. doi:10.1093/acprof:oso/9780195152968.001.0001
Skutle, A. (2017, January 1). Pasienttrender for perioden 2009–2016 – Demografi, rus og psykisk helse [Patient trends for the period 2009–2016 – Demography, substance abuse, and mental health]. Retrieved from https://bergensklinikkene.com/wp-content/uploads/2016/04/prosjekt-pasienttrender-2009-2016.pdf
Spitzer, R. (1983). Psychiatric diagnosis: Are clinicians still necessary? Comprehensive Psychiatry, 24(5), 399. doi:10.1016/0010-440X(83)90032-9
Tasca, G. A., & Gallop, R. (2009). Multilevel modeling of longitudinal data for psychotherapy researchers: I. The basics. Psychotherapy Research, 19(4–5), 429–437. doi:10.1080/10503300802641444
Thomas, V. H., Melchert, T. P., & Banken, J. A. (1999). Substance dependence and personality disorders: Comorbidity and treatment outcome in an inpatient treatment population. Journal of Studies on Alcohol, 60(2), 271–277. doi:10.15288/jsa.1999.60.271
Thylstrup, B., & Hesse, M. (2008). Substance abusers’ personality disorders and staff members’ emotional reactions. BMC Psychiatry, 8(1), 21. doi:10.1186/1471-244X-8-21
Toftdahl, N. G., Nordentoft, M., & Hjorthøj, C. (2016). Prevalence of substance use disorders in psychiatric patients: A nationwide Danish population-based study. Social Psychiatry and Psychiatric Epidemiology, 51(1), 129–140. doi:10.1007/s00127-015-1104-4
Trull, T. J., Jahng, S., Tomko, R. L., Wood, P. K., & Sher, K. J. (2010). Revised NESARC personality disorder diagnoses: Gender, prevalence, and comorbidity with substance dependent disorders. Journal of Personality Disorder, 24(4), 412–426. doi:10.1521/pedi.2010.24.4.412
Vélez-Moreno, A., Rojas, A. J., Rivera, F., Fernández-Calderón, F., Torrico-Linares, E., Ramírez-López, J., . . . Lozano, Ó. M. (2016). The impact of personality disorders and severity of dependence in psychosocial problems. International Journal of Mental Health and Addiction, 15(5), 1008–1022. doi:10.1007/s11469-016-9696-9
Verheul, R. (2001). Comorbidity of personality disorders in individuals with substance use disorders. European Psychiatry, 16(5), 274–282. doi:10.1016/S0924-9338(01)00578-8
Verheul, R., & van den Brink, W. (2005). Causal pathways between substance use disorders and personality pathology. Australian Psychologist, 40(2), 127–136. doi:10.1080/00050060500094613
Walter, M., Gunderson, J. G., Zanarini, M. C., Sanislow, C. A., Grilo, C. M., McGlashan, T. H., . . . Skodol, A. E. (2009). New onsets of substance use disorders in borderline personality disorder over seven years of follow-ups: Findings from the collaborative longitudinal personality disorders study. Addiction, 104(1), 97–103. doi:10.1111/j.1360-0443.2008.02413.x
Yen, S., Shea, T., Pagano, M., Sanislow, C. A., Grilo, C. M., McGlashan, T. H., . . . Gunderson, J. G. (2003). Axis I and Axis II disorders as predictors of prospective suicide attempts: Findings from the collaborative longitudinal personality disorders study. Journal of Abnormal Psychology, 112(3), 375. doi:10.1037/0021-843X.112.3.375
Zanarini, M. C., Frankenburg, F. R., Hennen, J., & Silk, K. R. (2003). The longitudinal course of borderline psychopathology: 6-year prospective follow-up of the phenomenology of borderline personality disorder. American Journal of Psychiatry, 160(2), 274–283. doi:10.1176/appi.ajp.160.2.274
Zanarini, M. C., Frankenburg, F. R., Weingeroff, J. L., Reich, B., Fitzmaurice, G. M., & Weiss, R. D. (2011). The course of substance use disorders in patients with borderline personality disorder and Axis II comparison subjects: A 10-year follow-up study. Addiction, 106(2), 342–348.