
Previous research indicates that the effects of terrorism vary across different parts of a population. Survivors of terrorism often have substantial psychological difficulties, physical injuries, and reduced day-to-day functioning (Dyb et al., 2014), and the bereaved can experience the death of a spouse, a child, or a close friend as a traumatic loss that may lead to a number of psychological problems, including post-traumatic stress reactions (PTSR) (Kristensen, Weisæth, & Heir, 2012). Research also indicates that the general population can experience acute stress symptoms, uncertainty, and fear of new attacks (Holman, Garfin, & Silver, 2014; Thoresen, Aakvaag, Wentzel-Larsen, Dyb, & Hjelmdal, 2012).
The terrorist attacks in Norway on July 22, 2011 were brutal in nature and profoundly shocked people both in Norway and internationally. The bomb in Oslo’s government quarters killed eight people, injured many, and caused significant material damage. On Utøya Island, 69 people were killed, most of whom were teenagers. The attack lasted for 70 minutes before authorities were able to detain the perpetrator. Both Norwegian and international media covered the attacks closely, publishing graphic pictures and videos of dead and injured victims as well as the terrorist acts themselves (Brurås, 2012).

Several studies investigating the effects of these attacks have been published in recent years (Dyb et al., 2014; Nordanger et al., 2013; Thoresen et al., 2012; Wollebæk, Enjolras, Steen-Johnsen, & Ødegård, 2012). While the results of these studies add to our understanding of how different parts of the Norwegian population reacted to terrorism, very few of them investigate the relationship between exposure to the attacks via media and mental health.
The aim of this study is to investigate whether the amount of media exposure to the terrorist attacks on Oslo and Utøya Island on July 22, 2011 can explain the variance in PTSR in a sample of parents.
Previous research and methodological issues
Studies investigating the relationship between media exposure to traumatic events and negative health consequences for the population receiving such exposure have found correlations between media exposure and PTSR (Ben-Zur, Gil, & Shamshins, 2012; Dougall, Hayward, & Baum, 2005; Lau, Lau, Kim, & Tsui, 2006; Silver et al., 2013), anxiety symptoms (Cohen et al., 2006), depression, and post-traumatic stress disorder (PTSD) (Ahern et al., 2002; Gershoff, Aber, Ware, & Kotler, 2010; Marshall, 2002). Research also indicates that the impact of media exposure on mental health problems varies across different parts of a population. An example of this tendency is an interaction between direct exposure to the terrorist attacks of September 11, 2001 and exposure to media coverage of these attacks (Ahern et al., 2002).
To achieve clear results in this field of study, controlling whether or not the sample has been directly exposed to the traumatic event is essential. Unfortunately, such control has not been common practice (Pfefferbaum, Pfefferbaum, North, & Neas, 2002). By not separating different parts of the population with entirely different traumatic experiences in the statistical analysis, the researcher risks the possibility that group affiliation functions as a moderating variable between media exposure and PTSR. Thus, the researcher could overestimate the relationship between these variables. Because of this tendency, the present study has divided its sample into two distinct groups: bereaved parents who lost a child in the attack on Utøya Island and a control group who did not lose any close relations in these attacks. Although this distinction limits the generalizability of our results to these specific groups, it also limits the influence of potential confounding variables on our results.
Previous research shows that the loss of close family members is associated with a wide array of mental illness including PTSD, depression, and complicated grief (Kristensen et al., 2012). These difficulties are also found to persist many years after the death. In a longitudinal study, Murphy et al. (1999) found that PTSD was prevalent in 21% of mothers and 14% of fathers two years after the death of their child. Because of this, it is reasonable to assume that many of the bereaved parents in our group are still showing high levels of PTSR today and that their level of PTSR is not comparable to that of the general Norwegian population (Ahern et al., 2002; Pfefferbaum et al., 2002). Despite this assumption, there are studies indicating that the general population can also experience negative health consequences after terrorist attacks.
In their study of the 2013 Boston City Marathon bombing, Holman and co-workers (2014) found a significant relationship between media exposure and acute stress symptoms for people who were solely exposed through the media and for those who were directly exposed to the attacks. They also found that people who were directly exposed to the attacks, later exposed themselves to more media than others. Similarly, Silver and co-workers (2013) found a relationship between media exposure after the terrorist attacks of September 11, 2001 and PTSR both two and three years after these attacks. Using a hierarchical regression model, these researchers showed that both acute stress and daily media exposure for four or more hours a day were significant predictors of PTSR experienced two and three years after the attacks (Silver et al., 2013).
Research questions and hypotheses
Considering the brutal nature of the attacks, the loss the bereaved have suffered, and the public accessibility of information concerning the deaths of their loved ones, it is reasonable to expect that the bereaved in our study have an elevated level of PTSR. Furthermore, it is also reasonable to assume that certain individuals in the general population can report elevated levels of PTSR after the attacks. To the authors’ knowledge, the effect of media exposure after the attacks of July 22, 2011 has not yet been investigated. Consequently, there is no knowledge of whether or not media exposure influenced the mental health of certain parts of the Norwegian population more than others.
This study aims to answer the following research questions: Is there a significant difference between the bereaved parents and a representative control group with regard to the amount of PTSR or the amount of media exposure? Can the amount of media exposure predict PTSR after the incident? And is the effect of media exposure higher in the bereaved group than in the control group? Our hypotheses are as follows:

- Hypotheses 1: The bereaved group will report a higher level of PTSR than the control group.
- Hypotheses 2: The bereaved group will report a higher level of media exposure than the control group.
- Hypotheses 3: Media exposure is a significant predictor for PTSR.
- Hypotheses 4: Media exposure will have a greater effect on the PTSR level in the group of bereaved parents than in the control group.
Method
Participants and procedure
The bereaved. Using publicly accessible lists, all parents and stepparents were sent an information letter and a declaration of consent. Consenting parents and stepparents then received pre-paid envelopes with questionnaires. The letters were sent to the bereaved parents at two time points. The first time point (T1) was 02/02/2013 and the second (T2) was 04/10/2013. At T1 the information letter and declaration of consent were sent to all of the 128 parents and stepparents. Of the 128 parents and stepparents, 67 responded that they would like to participate, and one father gave notice that he did not want to participate. The respondents who wished to participate all received a survey battery in mid-February 2013.
At T2, all 127 parents and stepparents were contacted again. The father who had given notice he did not want to participate was excluded. In addition to the 67 parents and stepparents who had already answered the survey, 19 more people wished to participate at this point. All of the surveys were sent out at the same time, between the second and fourth of October 2013. The average age of the respondents was 52.2 years old (SD: 6.9, range: 40–79), and the response rate was 67.2%. (View Table 1 for more demographic information about the participants.) The results of this study are mainly based on the data from T2.

Control group. The control group was selected through a stratified sampling of the Norwegian population. By using known response rates in the Norwegian population (Pallesen, Hanss, Mentzoni, Molde, & Morken, 2014), the number of respondents contacted was adapted to the number of bereaved based on the variables of gender and age. In addition, only people who were noted in the population registry as having children were contacted. In total, 293 people (133 men and 160 women) between the ages of 36–78 were selected from the population as potential participants in the control group. The IT company EVRY, through the Norwegian population registry, conducted a random selection of potential participants. All potential participants were sent an envelope with the survey battery, a pre-paid envelope, and an information letter. The response rate in the control sample was 22.9%. Of the 67 parents who replied (36.4% men), the average age was 49.9 years (SD: 6.01, range: 36–61).
Ethical considerations. For both groups, the information letter included a short description of the study’s intent, information that explained the participation as being voluntary, and assurance that the answers given were anonymous. Furthermore, the data were anonymized, and the respondents were given a phone number and an email address enabling them to contact the study coordinators in case of questions or if they were in need of any support or help from a healthcare professional. The survey batteries and the procedure used to collect the data from the two groups were evaluated and accepted by the Regional Ethics Committee.
Survey battery
The survey battery the bereaved received contained introductory texts referring directly to the terrorist attacks and the loss of a child. The survey battery the control group received was adapted through rewriting of these introductory texts and rewording, switching, or removing questions considered irrelevant for people who had not experienced loss in the attacks. Furthermore, questions concerning earlier loss and mental health were removed to limit any possible psychological stress on the participants. In addition to the questionnaires, the survey batteries contained demographic variables including age, gender, education, employment, and geographical location. In the main analysis, a media exposure scale developed by the Center for Crisis Psychology was used as a measure of how much time the respondents spent following media coverage of the attacks, and the Impact of Events Scale – Revised (IES-R) was used to measure the degree of PTSR.
Impact of Events Scale – Revised. IES-R is a 22-item self-report questionnaire designed to measure PTSR related to a specific event (Weiss & Marmar, 1997). The respondents are asked to judge if, and to what extent, their reactions over the last seven days match the different PTSR symptoms. The items are answered using a five point Likert scale graded as follows: not at all, a little, moderately, quite a lot, very much. The IES-R correlates highly with other measures of PTSD and has the ability to differentiate between groups that have and do not have PTSD consistently (Beck et al., 2008). In this study we operated with a centered average score of the IES-R.
Media exposure scale. The media exposure scale investigates how many hours informants spent on media coverage every day, at different points in time, after the terror attacks. The informants could answer: up to two hours, from two to four hours, or more than four hours. The answers were given in connection with their media consumption over the following time periods: «the first week after the terror on July 22nd,» «the following month,» «the time after the attacks until the beginning of the trial,» «the first week of the trial,» and «later during the trial.» A centered average score was used in the analysis as a measure of the participants’ total amount of media exposure after the attacks. The media exposure scale was developed in accordance with previously developed scales measuring media exposure after the terrorist attacks (e.g., after the attacks of September 11, 2001), but it has not been evaluated using psychometric testing.
Analysis
Two Chi-square tests where used to investigate whether or not the groups matched on gender distribution and education level. A two-tailed t-test for independent groups compared the age of the groups.
Since several of the variables were not normally distributed, a Mann-Whitney U test was performed to investigate the difference in PTSR and media exposure between the studied groups. A hierarchical multivariate regression analysis, using IES-R scores as the dependent variable, investigated how much of the variance in PTSR could be explained by the variable media exposure. The first model contained the variables education level, gender, and group. Before adding education level in model one, the variable was recoded from a categorical variable into two dummy variables. Initially the variable contained three levels: primary school, high school, and higher education. In the recoding, primary school was used as a reference score. The two dummy scores therefore compared the difference between having finished primary school and having finished high school, and the difference between having finished primary school and having finished some form of higher education.
In model 2, the amount of reported media exposure was added. To investigate if media exposure had a greater effect in the bereaved group than in the control group, an interaction variable between media exposure and group affiliation was added as a predictor in model 3.

In addition, two simple regression analyses were undertaken on the groups separately. Here, the predictors (i.e., gender, education, and amount of media exposure) were used to investigate whether or not media exposure was a significant predictor for PTSR in the groups as separate entities. Furthermore, the relationship between media exposure and PTSR for the two groups was plotted in a scatterplot (see Figure 1), which was used as an aid while interpreting the results (see discussion below). All the continuous variables used in the analysis were centered average scores, and the presumptions of homoscedasticity and independent and normally distributed residuals were tested and judged to be upheld.
Results
Descriptive analysis
The Chi-square tests showed that there was a significant difference between neither the groups’ gender distribution (X2 [1, N = 152] = 1.952, p = .162) nor their education level (X2 [2, N = 152] = 3.328, p = .189). In addition, the two-tailed t-test for independent groups showed that the control group’s age (M = 49.9, SD = 6.01) did not differ from the age of the bereaved (M = 52.2, SD = 6.90), t(150) = –1.96, p = .052, d = .32.
Main analysis
The results from the Mann-Whitney U test showed that the amount of media exposure reported by the control group (Mdn = 1.2) was significantly less than the amount of media exposure reported by the bereaved (Mdn = 1.6), U = 1682, z = –4.1, p = .000, r = –.33. This finding corresponds to a medium effect size. The control group also scored significantly lower (Mdn = 0.36) than the bereaved on IES-R (Mdn = 1.75) U = 663, z = –8.1, p = .000, r = –.66. This finding corresponds to a large effect size.
The multiple regression analysis (see Table 2) showed that media exposure was a significant predictor for IES-R score in both groups combined. Model 1, where gender, education, and group affiliation were used as predictors, explained 47.1% of the score’s variance. By adding media exposure in model 2, the explanatory strength of the model increased by 2.5% to 49.6%.
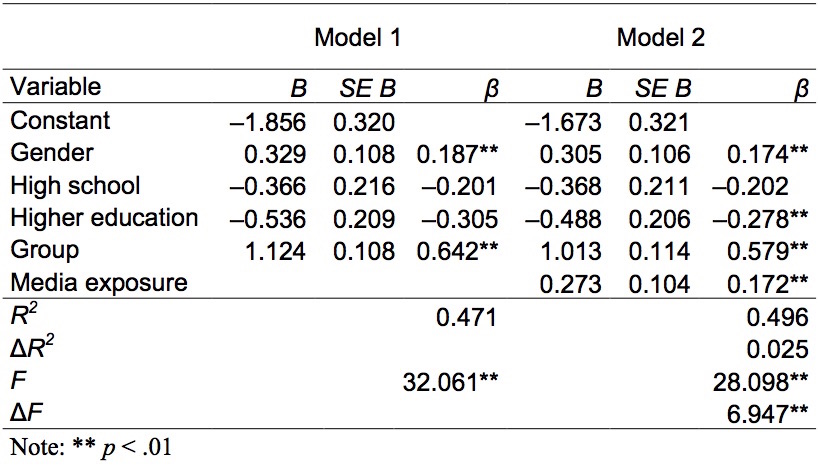
The third model did not explain significantly more than model 2 (ΔF [1, N = 142] = 1.624, p = .205) and the interaction between media exposure and group affiliation was not a significant predictor β = 0.369, t(142) = 1.77, p = .205. This result implies that media exposure did not have a significantly higher predictive ability in the group of bereaved than in the control group.
The two single regression analyses showed that gender, education, and media exposure were not significant predictors for PTSR in the control group (see Table 3), but all of these variables were significant predictors for PTSR in the bereaved group, explaining 23.4% of the variance in PTSR.

Discussion
In this study, the group of bereaved parents reported a higher degree of PTSR and a higher degree of media exposure than the control group following the terrorist attacks in Norway on July 22, 2011. The amount of media exposure reported was found to be a significant predictor for PTSR in both groups combined. When this analysis was conducted on each group separately, media exposure was found to be a significant predictor of PTSR in the bereaved group but not in the control group. This last result contradicts both our third and fourth hypotheses. It also contradicts previous research in the area, which has shown media exposure as a predictor for PTSR in groups similar to this study’s control group (Ben-Zur et al., 2012; Dougall et al., 2005; Lau et al., 2006; Silver et al., 2013). These findings show us seemingly contradictory results. On the one hand, our data tells us that media exposure cannot predict PTSR variance in the control group alone, but it can in the bereaved group. On the other hand, our data tells us that there is no difference between these groups in media exposure’s ability to predict PTSR.
There are several possible explanations for this contradiction. One simple explanation would be that the attacks on Utøya Island, and the resulting media coverage, did not have the same effect on our sample as in other samples used in similar studies. This inconsistency could be due to cultural differences or differences in how the attacks were conducted or handled. However, such theories do not tell us what effect the attacks and media coverage did have. If we look at the scatterplot created to visualize the results (see Figure 1), it shows that the trend in the regression line is a rising slope similar to that of the bereaved group’s regression line.

Assuming this trend points to a connection between media exposure in the control group as well, a lack of statistical power could explain why media exposure is not considered a significant predictor in our control group. If statistical power is a problem, it is not possible to determine whether both the third and fourth hypotheses would be supported or if the results would lend support to either one in isolation.
Regression analysis allows us to estimate how well one or more variables can predict another, but it is still important to note that these analyses tell us nothing about the causal direction of our findings. One possibility is that media exposure caused parts of the PTSR in the sample, but it is equally possible that these results are due to people with a higher level of PTSR exposing themselves to a larger amount of media coverage compared to people with lower PTSR levels. A third possibility is that there is a mutual influence between the variables. In this way, people with higher degrees of PTSR expose themselves to larger amounts of media coverage, and this tendency in turn elevates their PTSR. As a group, the bereaved in our sample report a significantly higher level of media exposure than the control group. This tendency has previously been observed in people who were present during the terrorist attack in Boston compared to people who were not present (Holman et al., 2014). The reason for this is not apparent in our analysis, but a possible explanation may be that the bereaved in our sample used the media coverage to better make sense of their loss and to gain information about the event. Given that many of the bereaved had to wait several days before the lists of the people who lost their lives were made available (Strand, 2014), it can be assumed that they utilized the media as a resource to gain knowledge about their child.

Previous studies on the subject show that bereaved people who have experienced loss as a result of murder show a higher degree of complicated grief and PTSD compared to those bereaved by suicide or accidents (Currier, Holland, & Neimeyer, 2006; Kristensen et al., 2012; Murphy, Johnson, Wu, Fan, & Lohan, 2003). A possible explanation for these findings could be that murder-related deaths and subsequent trials are often covered closely by the media, while accident- and suicide-related deaths are not (Kristensen et al., 2012). This explanation suggests that the more public a death becomes through media coverage, the more painful reminders, including brutal details of how the murder was committed, are made available to the bereaved. Applying this theory to the attacks on Oslo and Utøya, it is clear that the subsequent media coverage of the attack, the trial, and debates about the sanity of the perpetrator might have contributed to an even higher level of suffering in the bereaved group. In connection to the terror attacks of September 11, 2001, the «International Society for Traumatic Stress Studies» (ISTSS) recommended that people with previous traumatic experiences should shield themselves from media coverage of the terrorist attacks (Putnam, 2002). Our results support this recommendation; however, the same recommendation does not seem necessary for people exposed to trauma through the media alone.
Limitations
The surveys used were not the same in the two groups and this discrepancy could make a comparison of the groups less informative than if the surveys were identical. However, all the changes made were necessary for the surveys to make sense to the informants and to enable us to collect relevant information from each group. Nevertheless, several variables that were not measured might have given greater insight into the effects of media exposure. For example, the questionnaires did not differentiate between disturbing coverage of the terror attacks and coverage concerning conciliatory events like commemorative concerts or support marches. Furthermore, the media exposure scale did not give the option of reporting complete avoidance of all media coverage, and it is unknown how accurately the media exposure scale can measure the amount of media the participants actually viewed. Nonetheless, it is important to note that our analysis is dependent on a rank difference between participants and is not a measurement of exact time spent on media coverage related to the attacks. Still, it is possible that adding these nuances to the analysis could have benefited the study by providing a deeper understanding of the effects of media consumption after similar catastrophes.
The PTSR scores from the bereaved were collected nine to 10 months prior to the control group’s PTSR scores. Because of practical considerations, this delay was unavoidable. The media exposure questions were nonetheless related to the same time periods for both groups. Because we weren’t able to compare the groups’ PTSR levels at the same point in time, it is possible that the difference in PTSR levels is a function of time alone. In addition, the difference in time allows for other confounding variables to affect only one of the groups in isolation. An example of this is that the data from the control group was collected at the beginning of August 2014, three weeks after the three-year commemoration of the terrorist attacks on Oslo and Utøya. Previous research has shown that commemoratory dates may elevate the symptom levels in the general population. For example, Cohen and coworkers (2006) showed such a tendency at the one- and two-year commemorations of the terrorist attacks committed on September 11, 2001. In addition to being in close proximity to the commemorative date, there was an ongoing terror threat that gathered great media coverage in Norway in the weeks preceding data collection from the control group. Finally, the control group data may be affected by a response bias, whereby the people experiencing the most severe symptoms are more inclined to answer the survey.
In spite of these shortcomings, the study utilizes data collected with a high response rate for the bereaved. It is therefore considered to give a valid measure of the bereaved group’s reactions. The response rate in the control group coincides with the expectations at the time of collection, and the control group is also a good match for the bereaved. With this in mind, the data collected from the control group is regarded as a representative and valid measure of their reactions. Furthermore, the separation of the two groups allows for an investigation of the effect of media exposure in isolation rather than under the influence of group affiliation. In sum, the study has a good design that allows for the comparison of the two groups. However, the difference in the time of data collection between the groups may have allowed confounding variables to affect the groups unevenly. Any possible consequences of this contingency are unknown.
Recommendations for future research
Based on the recommendation of previous studies on the effects of media exposure (Pfefferbaum et al., 2002), we distinguished between parents of victims (bereaved) and people who had not lost a close relative (control group). Our results indicate a clear difference between these two groups. Since this has not been common practice (Pfefferbaum et al., 2002), we recommend that future researchers continue to distinguish between these groups.
The bereaved report a higher level of PTSR and media exposure than the control group.
Conclusion
The results of this study show that the amount of time spent following the media coverage in the wake of the July 22, 2011 terrorist attacks is a significant predictor of PTSR in the bereaved. In addition, the bereaved report a higher level of PTSR and media exposure than the control group. These are significant differences between the bereaved and the general population, and not distinguishing between these groups could create serious methodological difficulties. Since this distinction has not always been made, we recommend that the two groups be separated in future research
After September 11, 2001, it was recommended that people who had lost a relation limit their exposure to media coverage of the attack. Our results support this recommendation. However, since the results of our analysis do not show that media exposure in itself causes prolonged traumatic reactions in people who have not lost a close relation, there is no empirical foundation for a recommendation to limit media exposure within the general population.
References
Abenhaim, L., Dab, W., & Salmi, L. R. (1992). Study of civilian victims of terrorist attacks (FRANCE 1982–1987). Journal of Clinical Epidemiology, 45(2), 103–109. doi: 10.1016/0895-4356(92)90002-5.
Ahern, J., Galea, S., Resnick, H., Kilpatrick, D., Bucuvalas, M., Gold, J., & Vlahov, D. (2002). Television images and psychological symptoms after the September 11 terrorist attacks. Psychiatry: Interpersonal and Biological Processes, 65(4), 289–300. doi: 10.1521/psyc.65.4.289.20240.
Beck, J. G., Grant, D. M., Read, J. P., Clapp, J. D., Coffey, S. F., Miller, L. M., & Palyo, S. A. (2008). The Impact of Events Scale-Revised: Psychometric properties in a sample of motor vehicle accident survivors. Journal of Anxiety Disorders, 22(2), 187–198. doi: 10.1016/j.janxdis.2007.02.007.

Ben-Zur, H., Gil, S., & Shamshins, Y. (2012). The relationship between exposure to terror through the media, coping strategies and resources, and distress and secondary traumatization. International Journal of Stress Management, 19(2), 132–150. doi: 10.1037/a0027864.
Bonanno, G. A., Rennicke, C., & Dekel, S. (2005). Self-enhancement among high-exposure survivors of the September 11th terrorist attack: Resilience or social maladjustment? Journal of Personality and Social Psychology, 88(6), 984–998. doi: 10.1037/0022-3514.88.6.984.
Brurås, S. (2012). Mediene og terroraksjonen: studier av norske mediers dekning av 22. juli. Oslo: Unipub.
Cohen, P., Kasen, S., Chen, H., Gordon, K., Berenson, K., Brook, J., & White, T. (2006). Current affairs and the public psyche: American anxiety in the post 9/11 world. Social Psychiatry & Psychiatric Epidemiology, 41(4), 251–260. doi: 10.1007/s00127-006-0033-7.
Currier, J. M., Holland, J. M., & Neimeyer, R. A. (2006). Sense-making, grief, and the experience of violent loss: Toward a mediational model. Death studies, 30(5), 403–428. doi: 10.1080/07481180600614351.
Dougall, A. L., Hayward, M. C., & Baum, A. (2005). Media exposure to bioterrorism: stress and the anthrax attacks. Psychiatry, 68(1), 28–42. doi: 10.1521/psyc.68.1.28.64188.
Dyb, G., Jensen, T. K., Nygaard, E., Ekeberg, Ø., Diseth, T. H., Wentzel-Larsen, T., & Thoresen, S. (2014). Post-traumatic stress reactions in survivors of the 2011 massacre on Utøya Island, Norway. The British Journal of Psychiatry, 204(5), 361–367. doi: 10.1192/bjp.bp.113.133157.
Dyregrov, K., Dyregrov, A., & Kristensen, P. (2014). Traumatic bereavement and terror: The psychosocial impact on parents and siblings 1.5 years after the July 2011 terror killings in Norway. Journal of Loss and Trauma, 20(6), 1-21. doi: 10.1080/15325024.2014.957603.
Franz, V. A., Arnkoff, D. B., Glass, C. R., Mete, M., & Dutton, M. A. (2011). Predictors of the impact of the September 11th terrorist attacks on victims of intimate partner violence. Journal of Traumatic Stress, 24(5), 530–537. doi: 10.1002/jts.20676.
Gershoff, E. T., Aber, J. L., Ware, A., & Kotler, J. A. (2010). Exposure to 9/11 among youth and their mothers in New York City: enduring associations with mental health and sociopolitical attitudes. Child Development, 81(4), 1142–1160. doi: 10.1111/j.1467-8624.2010.01459.x.

Hoffman, B. (2013). Inside Terrorism. New York: Columbia University Press.
Holman, E., Garfin, D. R., & Silver, R. C. (2014). Media’s role in broadcasting acute stress following the Boston Marathon bombings. PNAS Proceedings of the National Academy of Sciences of the United States of America, 111(1), 93–98. doi: 10.1073/pnas.1316265110.
Johnsen, I., Laberg, J. C., Matthiesen, S. B., Dyregrov, A., & Dyregrov, K. (2015). Psychosocial functioning after losing a close friend in an extreme terror incident. Scandinavian Psychologist, 2, e5. doi: 10.15714/scandpsychol.2.e5.
Kristensen, P., Weisæth, L., & Heir, T. (2012). Bereavement and mental health after sudden and violent losses: a review. Psychiatry: Interpersonal & Biological Processes, 75(1), 76–97. doi: 10.1521/psyc.2012.75.1.76.
Lau, J. T., Lau, M., Kim, J. H., & Tsui, H. Y. (2006). Impacts of media coverage on the community stress level in Hong Kong after the tsunami on 26 December 2004. Journal of Epidemiology and Community Health, 60(8), 675–682. doi: 10.1136/jech.2005.041897.
Lawyer, S. R., Resnick, H. S., Galea, S., Ahern, J., Kilpatrick, D. G., & Vlahov, D. (2006). Predictors of peritraumatic reactions and PTSD following the September 11th terrorist attacks. Psychiatry: Interpersonal and Biological Processes, 69(2), 130–141. doi: 10.1521/psyc.2006.69.2.130.
Marshall, R. D. (2002). If we had known then what we know now: a review of local and national surveys following September 11, 2001. Cns Spectrums, 7(9), 645–649.
Murphy, S. A., Braun, T., Tillery, L., Cain, K. C., Johnson, L. C., & Beaton, R. D. (1999). PTSD among bereaved parents following the violent deaths of their 12‐to 28‐year‐old children: A longitudinal prospective analysis. Journal of Traumatic Stress, 12(2), 273–291. doi: 10.1023/A:1024724425597.
Murphy, S. A., Johnson, L. C., Wu, L., Fan, J. J., & Lohan, J. (2003). Bereaved parents’ outcomes 4 to 60 months after their children’s deaths by accident, suicide, or homicide: a comparative study demonstrating differences. Death Studies, 27(1), 39–61. doi: 10.1080/07481180302871.
Nordanger, D. Ø., Hysing, M., Posserud, M. B., Lundervold, A. J., Jakobsen, R., Olff, M., & Stormark, K. M. (2013). Posttraumatic responses to the July 22, 2011 Oslo terror among Norwegian high school students. Journal of Traumatic Stress, 26(6), 679–685. doi: 10.1002/jts.21856.

Pallesen, S., Hanss, D., Mentzoni, R. A., Molde, H., & Morken, A. M. (2014). Omfang av penge- og dataspillproblemer i Norge 2013. Bergen, Norge: Universitetet i Bergen.
Pfefferbaum, B. (2003). Victims of terrorism and the media. In A. Silke (Ed.), Terrorists, victims, and society: Psychological perspectives on terrorism and its consequences (pp. 175–187). Hoboken, NJ: Wiley.
Pfefferbaum, B., Pfefferbaum, R. L., North, C. S., & Neas, B. R. (2002). Does television viewing satisfy criteria for exposure in posttraumatic stress disorder? Psychiatry: Interpersonal and Biological Processes, 65(4), 306–309. doi: 10.1521/psyc.65.4.306.20242.
Putnam, F. W. (2002). Televised Trauma and Viewer PTSD: Implications for Prevention. Psychiatry: Interpersonal and Biological Processes, 65(4), 310–312. doi: 10.1521/psyc.65.4.310.20241.
Saylor, C., DeRoma, V., & Swickert, R. (2006). College students with previous exposure to crime report more PTSD after 9-11-2001. Psychological Reports, 99(2), 581–582.
Silver, R. C., Holman, E., Andersen, J. P., Poulin, M., McIntosh, D. N., & Gil-Rivas, V. (2013). Mental- and physical-health effects of acute exposure to media images of the September 11, 2001, attacks and the Iraq war. Psychological Science, 24(9), 1623–1634. doi: 10.1177/0956797612460406.
Slone, M., Shoshani, A., & Baumgarten-Katz, I. (2008). The relation between actual exposure to political violence and preparatory intervention for exposure to media coverage of terrorism. Anxiety, Stress, & Coping, 21(3), 243–261. doi: 10.1080/10615800701510124.
Strand, N. (2014). Partisekretærens ukjente 22. juli-historie. Tidsskrift for Norsk Psykologforening, 51(7), 546–558.
Thoresen, S., Aakvaag, H. F., Wentzel-Larsen, T., Dyb, G., & Hjelmdal, O. K. (2012). The day Norway cried: Proximity and distress in Norwegian citizens following the 22nd July 2011 terrorist attacks in Oslo and on Utøya Island. European Journal of Psychotraumatology, 3. doi: 10.3402/ejpt.v3i0.19709.
Weiss, D. S., & Marmar, C. R. (1997). The impact of event scale-revised. Assessing Psychological Trauma and PTSD, 2, 168–189.
Wollebæk, D., Enjolras, B., Steen-Johnsen, K., & Ødegård, G. (2012). After Utøya: how a high-trust society reacts to terror—trust and civic engagement in the aftermath of July 22. PS: Political Science & Politics, 45(1), 32–37. doi: 10.1017/s1049096511001806.